All of my patients get a one time Lp(a), I don’t see a value in repeating it, as I target APOB to 70’s if low, or 50’s if high. If someone already has established disease however, pushing it lower than these targets is my current approach.
If obicetrapib gets approved next year (or whenever), would you expect to be prescribing it for individuals with high LP(a) and established disease?
Some of us have seen quite large deltas
See eg
So it seems like it might actually be good to measure more than once
(Question is if it’s measurement error or if we actually hanging them by our activities…)
I’m getting mine rechecked at a different lab (Quest) this Friday, since I no longer trust the lab that was doing it before.
Effects of Exercise on Lipoprotein(a)
Recent intervention studies also suggest that 9 to 12 months of intense exercise training may elevate serum Lp(a) levels. However, these changes are generally modest (10 to 15%) and, in most individuals, serum Lp(a) levels remain within the recommended range. It is unclear whether increased serum Lp(a) levels after intense exercise training are of clinical relevance, and whether certain Lp(a) isoforms are more sensitive to the effects of exercise training. Since elevation of both low density lipoprotein cholesterol (LDL-C) and Lp(a) levels in the blood exerts a synergistic effect on cardiovascular disease risk, attention should focus on changing lifestyle factors to decrease LDL-C (e.g. dietary intervention) and increase high density lipoprotein cholesterol (e.g. exercise) levels in the blood.
https://doi.org/10.2165/00007256-199928010-00002
This article would suggest a 10-15% change might occur with lifestyle changes/activity - but we’d not expect 100% or in the case above 300% changes.
Yes, but it’s happening in the data - so then the test is noisy? I’d so seems like more than one year is needed and look at averages and ranges to guide?
No 10-15% change won’t change anything - I have lots of patients simply with a Lp(a)<10. I guess the folks in the middle with 50-70 might be worth trending - but usually the folks who are high, are pretty clearly high e.g. 120-200 … so a 10-15% variation wouldn’t change the treatment target on the ApoB.
It is interesting that individuals are seeing such huge variations in results - it shouldn’t be the case.
I’m talking about the 100% deltas in the blood work, not the 15% that diet can move.
If I only had my lowest value I would not be that concerned
If I only had my highest value I would def take it seriously
With only one test result I would not have a good sense or a false sense of where I am on this risks factor
I’d go with the Quest CardioIQ Lp(a) as a good consistent choice. I’m sure there are others but I’ve been happy with that one.
Yes the massive variation has me more concerned about lab errors as it shouldn’t vary like that.


I’ve mostly used Quest. Thought CardioIQ was same assays, just that IQ provides some more visualizations, etc. Is it actually a different test/measurement assay?
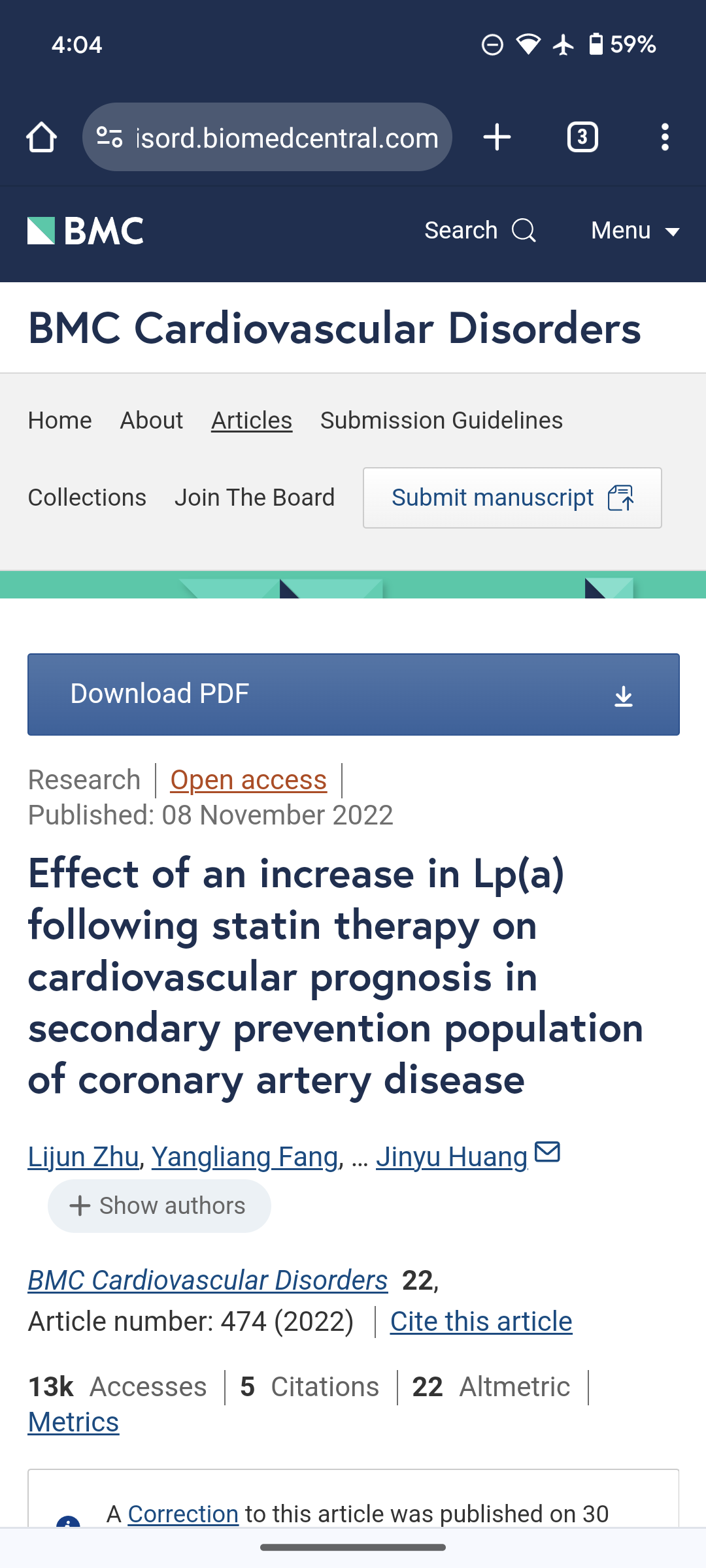
My Quest results since 2018:
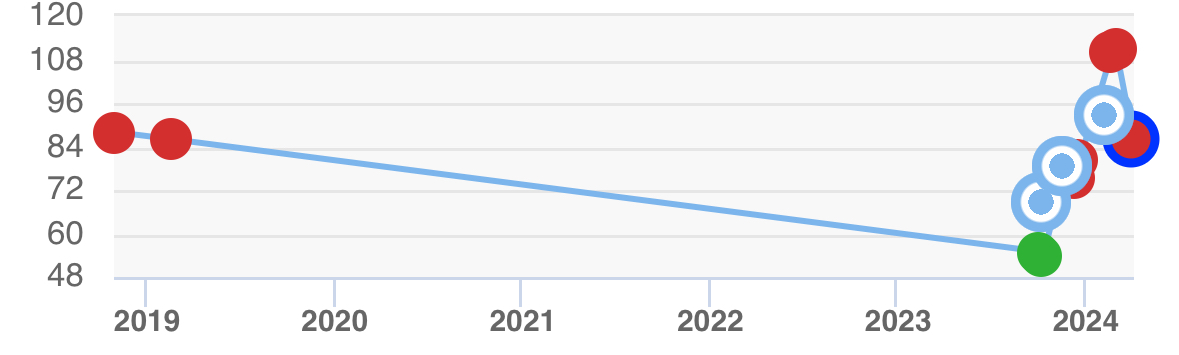
And roughly the last 6 months:
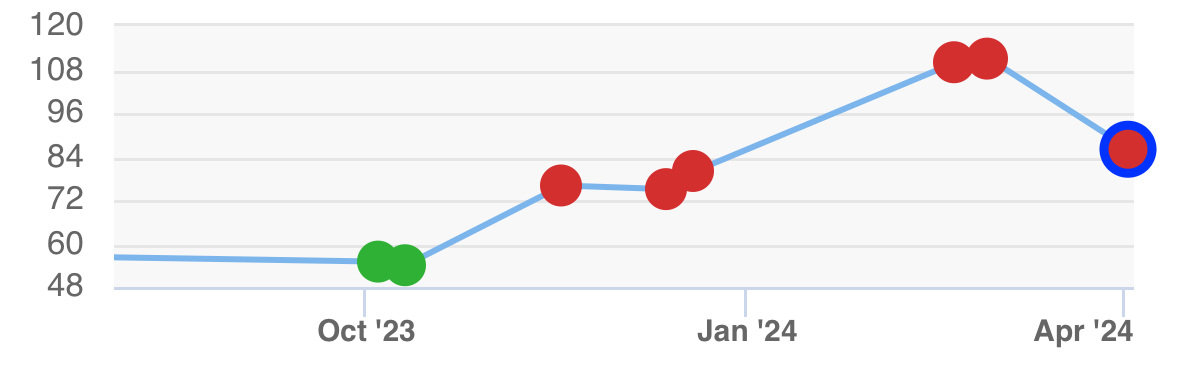
There is perhaps some influence of age on levels (but doubt that is driving these huge moves in short time periods):
One thing I’ve wondered about is the effect (if any) of SGLT2 inhibitors on Lp(a). We know these drugs can raise LDL to some degree, although it appears this may be due a shift from small dense LDL particles to large LDL particles (a beneficial effect). I haven’t seen anything looking at Lp(a) in 'flozin users, and I’ve been off/on cana and empa for the last couple of years. I’ve been much more consistently taking empagliflozin over the past 6 months and plan to continue, but I do wonder if the empa has anything to do with my Lp(a) changes.
(Review of SGLT2i drugs and lipid metabolism, bit no mention of Lp(a))
For folks with these huge fluctuations… which I’d say are totally not expected … was there any timing of changes with meds or supplements? Maybe it is lab issues, but it would be a worry if in our pursuit of living longer some things we are doing are pushing this up dramatically.
Don’t know what to think, don’t have an explanation for fluctuations of a magnitude that plainly shouldn’t occur.
What is a huge fluctuation?
We don’t expect more than 10 to 20% normally. Mine have been <10 … nothing different ever reported … have only measured twice as this should be a 1 time only test in most circumstances
Here are the values I have had (normally at least 2 weeks or more apart, but sometimes every 2 weeks)
8.2, 7.8, 5.7, 5.3, 13, <5.2, 5.5, 5.8, 5.6,7.1,5.8, 5.5 nmol/l and previously 39.4, 31.3, <30.0 mg/l
I think 30 mg/l is 12 nmol/l
So not huge variations - none of these would result in differing advice to a patient. Having values like 50 mg/dL where things are okay - and next thing have 180 mg/dL is where the problem is - because that makes a massive change in where one would target their APOB. Your values are all consistent with not being concerned about your Lp(a).
LP(a):
109.7 on 5/19/21 ( LabCorp)
106.4 on 6/21/22 (LabCorp)
Started taking rosuvastatin 5 mg and ezetimibe 10 mg end of 2022
LP(a): 151 on 10/20/23 (Quest)
Increase of about 40% between 6/22 and 10/23. Could have been use of stain/ezetimibe and/or different lab. Either way, 40% delta does not fit well with genetically determined.
Some studies have shown an increase of 10-20% in LP(a) with statin use. E.g: