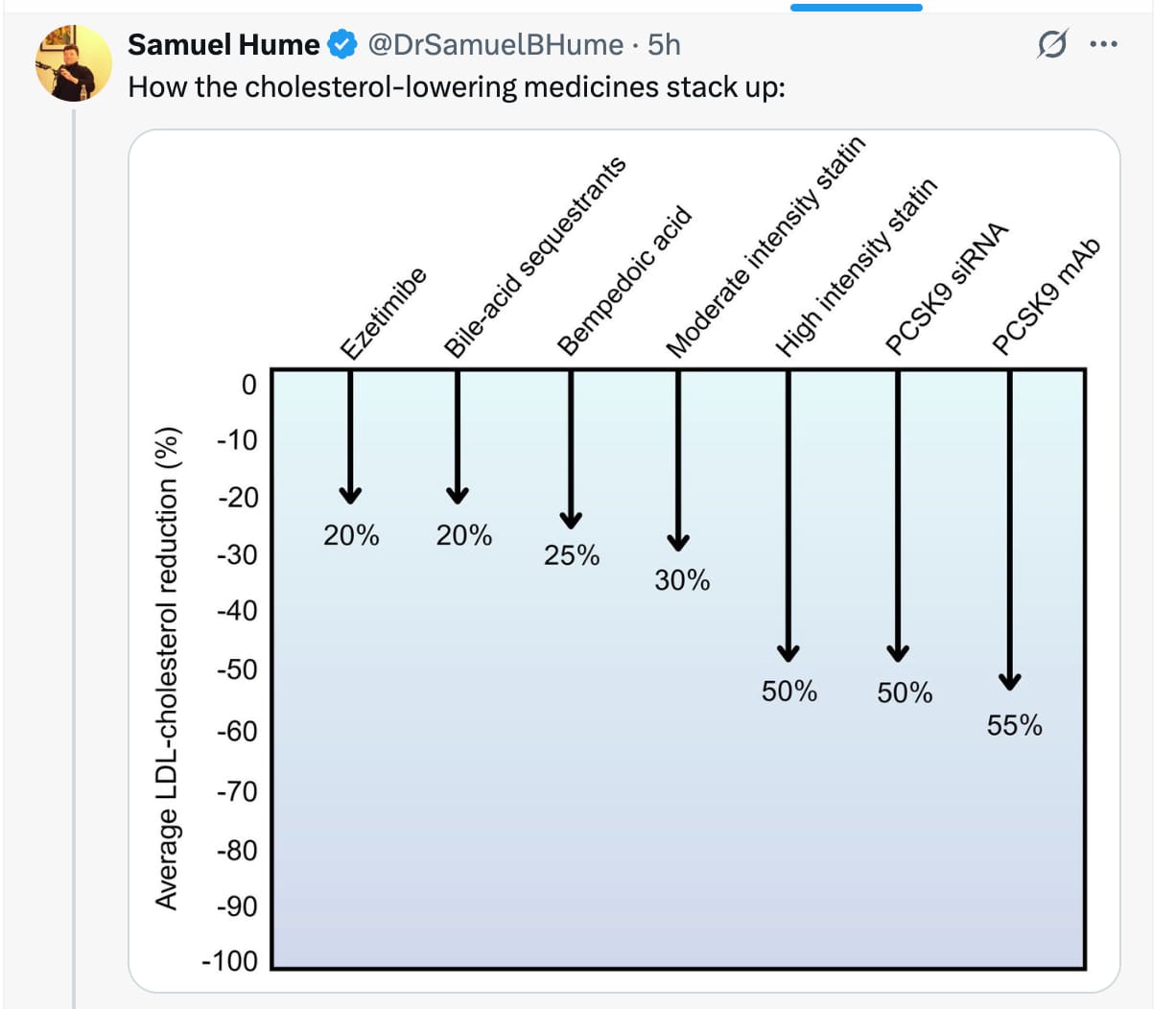
I had not seen this presented this way… seems about right.
7 Likes
I really like this, and I’d love to see it extended with some dietary/lifestyle data.
I don’t have % data on everything but:
Mod resistance Exercise => 50 mg/dl reduction in apob
Soluble fibre 20g extra per day => 22mg/dl reduction in ldlc
Fish x2 weekly => 23% reduction in apob
20ml of EVOO 8% reduction in apoB
Nuts 43g of walnuts a day => 7 mg/dl reduction in apob
4 Likes
“In statin-free patients with type 2 diabetes, the combo cut LDL-C ~39% vs ezetimibe ~19%”
"Effect of bempedoic acid plus ezetimibe fixed-dose combination vs ezetimibe or placebo on low-density lipoprotein cholesterol in patients with type 2 diabetes and hypercholesterolemia not treated with statins - PMC’
4 Likes
And possibly the statins affects on sirt 6. Such as for atorvastatin, just googling:
AI Overview
Atorvastatin (a statin) directly suppresses Sirtuin 6 (SIRT6) expression in the liver by increasing a microRNA called miR-495, leading to increased activity of the FoxO1 gene and enhanced gluconeogenesis (sugar production). While SIRT6 generally promotes metabolic health and has anti-fibrotic effects, this statin-induced reduction of SIRT6 contributes to statin-associated hyperglycemia and may present a therapeutic target to prevent this side effect.
Atorvastatin’s effect on SIRT6:
Direct repression: Atorvastatin and other statins directly lower SIRT6 protein levels.
miR-495 induction: This occurs because statins increase the expression of miR-495, a microRNA that directly inhibits SIRT6.
Consequences of reduced SIRT6:
Increased FoxO1 activity: With lower SIRT6, the FoxO1 protein becomes more active.
Enhanced gluconeogenesis: Increased FoxO1 activity stimulates genes involved in producing glucose in the liver.
Statin-induced hyperglycemia: The combined effect of reduced SIRT6 and increased gluconeogenesis contributes to the high blood sugar that can be a side effect of statin therapy.
SIRT6’s normal role:
Metabolic regulation:
SIRT6 is known to play a protective role in liver health and metabolic homeostasis.
Anti-fibrotic effects:
It helps prevent liver fibrosis and inflammation by regulating pathways like TGF-β.
Lipid regulation:
SIRT6 is also involved in regulating cholesterol and low-density lipoprotein (LDL).
Therapeutic Implications:
Preventing side effects:
.
Activating SIRT6, perhaps through specific activators, could be a way to prevent or mitigate statin-induced hyperglycemia.
It’s expensive, but it’s another reason I like donotage’s sirt 6, despite its lack of relative affordability. There have been some studies that may point to taking a sirt 6 activator to counteract some of these statin affects, which is why I take donotage’s product with the statin Statin suppresses sirtuin 6 through miR-495, increasing FoxO1-dependent hepatic gluconeogenesis - PMC
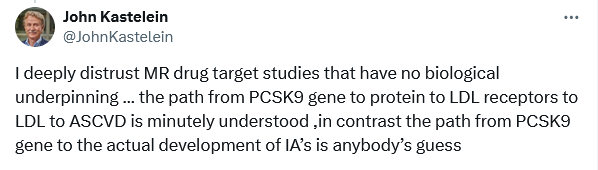
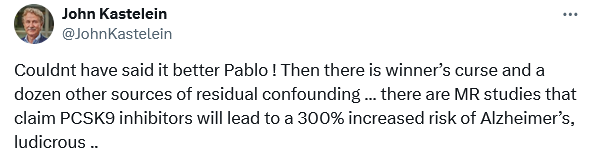
I don’t get it. He published an MR study on CETPi and dementia risk: Lower activity of cholesteryl ester transfer protein (CETP) and the risk of dementia: a Mendelian randomization analysis | Alzheimer's Research & Therapy | Full Text
Is it that when results aren’t aligned with his theory he’s against MR?
2 Likes
2 Likes
I presume (not speaking for him) he would claim that the CEPT pathway is well established, but PCSK9 is not (for dementia). The general point is valid, MR studies are only meaningful if the whole pathway is well understood, otherwise there are too many variables. Whether that’s the case with CEPT I don’t know, as I have not looked at that for dementia.
2 Likes
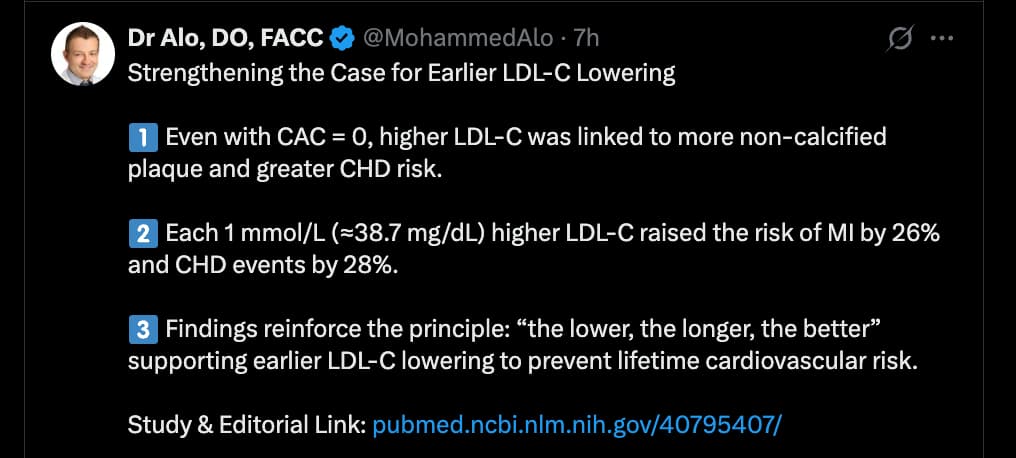
Get Lower, Faster…
source:
Strengthening the case for earlier LDL cholesterol lowering
and
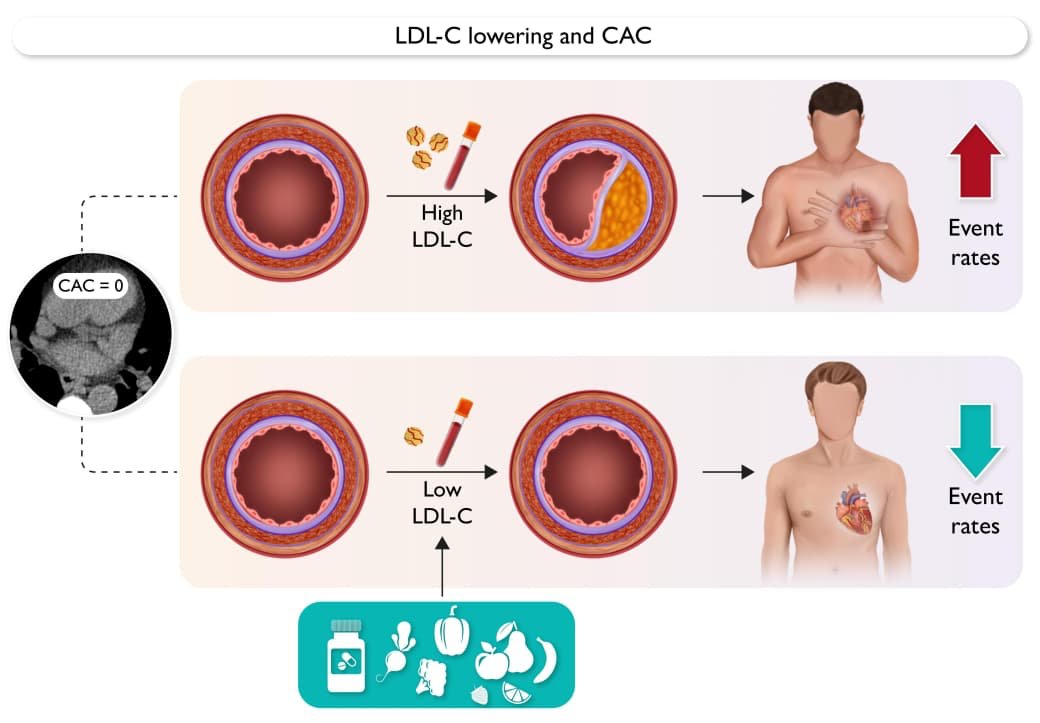
Conclusion: In symptomatic individuals with CAC = 0, elevated LDL-C is associated with higher risk of non-calcified plaque and with higher relative risk of future CHD events, most pronounced at age ≤45 years. This indicates that LDL-C control over a long-time horizon remains important in younger individuals despite CAC = 0.
5 Likes
I am also really interested in these sort of data. However, the big caveat is that the things depend a lot on your genetics, and the reasons for your high cholesterol.
Like, fish 2x per week for a 23% reduction is a crazy return on investment. That’s like a moderate intensity statin. Moderate resistance exercise too, if the 50mg/dl lowering is true.
I could imagine those being plausible for people whose starting point is a horrible diet and sedentary lifestyle. If they drastically turned around their diet, exercise, lifestyle (and obviously will lose weight, clear up fatty liver and other related things) then I could see those numbers coming true. But I am overall sceptical.
My own story is that I learned I had high cholesterol in my 20’s. I was actually into bodybuilding, so I had above average muscle, below average body fat, exercised regularly, and I controlled my diet very well. Doctor gave me the usual “eat less fat” story and assured me that my risk was low. She even pulled out the qRisk 10y calculator to show it…
Long story short, I have a genetic condition (familial hypercholesterolemia - mine is heterozygous, HeFH), and it turns out that this isn’t even particularly rare. ~1/200 people means more than 1M people in the USA will have shitty lipids, no matter what they do. UK data says that only 8% of people with HeFH are diagnosed. So I just caution against these sort of “lifestyle trumps everything” ideas because they don’t apply to everybody.
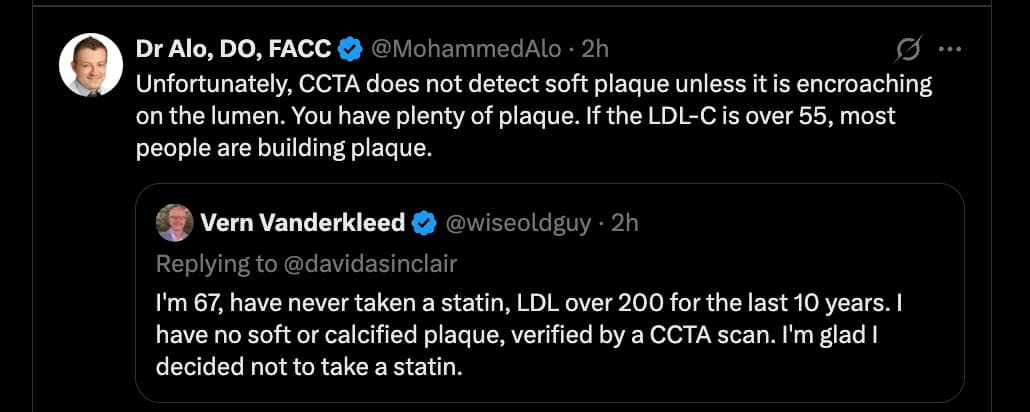
@RapAdmin For the last tweet from “wiseoldguy”, he might just be lucky. From what I know, some people are just really good at clearing plaque and don’t accumulate it. Maybe to do with their HDL-C activity, their immune system, or other aspects of their overall vascular inflammation. And if the guy is 67 and has a clean CTCA, he’s doing better than average and he’ll probably not die earlier than average from ASCVD. It obviously doesn’t mean it’s a good idea to leave your LDL-C >200.
5 Likes
Fully agreed. No matter what I did with diet, exercise and supplements, my LDL remained high - 160-180 mg/dL. And believe me, I went to extraordinary lengths. I was on CR for eight years, a lot of it pretty severe 1200-1400 cal/day… LDL remained high throughout. Fiber? Lol. Well over 100g/day. No difference. I did everything in the book, and chased down even very obscure remedies. Nothing doing.
If you have genetically high LDL, you simply can’t do squat without drugs. And even on 10mg/day atorvastatin, my LDL was 146 mg/dL. Now I’m trying Pitavastatin 4mg, equivalent of atorvastatin 20mg, adding either ezetemibe or bempedoic acid to the pita barely moved the needle. Now I’m trying pita+EZ+BA… we’ll see. I’m considering PCSK9i, but really I’m waiting for new drugs.
Again, it’s fine to advocate lifestyle and non pharma approaches to dislipidemia, but be aware that for a substantial number of people, these are useless.
6 Likes
I totally agree. The average statistical impact of any intervention on ldlc is always only motivator to try something. Testing post intervention is a must IMHO.
That obviously goes for both pharma and lifestyle. My strategy has always been lifestyle first then pharma. So the cost for anyone with FH trying that is only 6 months or so wasted time, waiting to see the impact of the lifestyle changes.
What drug combo is working for you? Are you on a statin + ezetimibe? Or a Psk9i?
Yeah, I did try following the doctors advice about lifestyle, but obviously to no effect.
In the end, statin + ezetimibe took my LDL-C to around 75kg/dl, and Repatha 140mg one per month (off-label dose protocol) gives me an average of 45-ish.
Yeah, this is another thing where I just have to assume there is a massive under-diagnosis. I saw the figure that only 8% of people with HeFH in the UK are actually diagnosed and under any sort of treatment. SO you have 70 millions people, ~1/200 (supposedly) with HeFH = 350,000 people, and 322,000 of them are currently untreated. That’s a lot of early MI and strokes that could be avoided. And all of them will have time wasted seeing a GP, getting bland advice about their diet and exercise, waiting for more blood tests, having the GP scold them for not dieting hard enough, or not taking their pills. When a statin didn’t budget my LDL-C at all, my doctor accused me of not being diligent enough with taking the medication.
6 Likes