No, I was simply illustrating that moderate to high egg consumption is not harmful to everyone.
The studies on egg consumption are a mixed bag and not very compelling. There are many confounding factors, and high egg consumption might be harmful to some people.
“The associations between egg consumption and the incidence of cancer, diabetes, cardiovascular diseases and other possibly related diseases have been assessed in numerous meta-analyses. However, in many cases several systematic reviews on the same subject, often only of low or moderate quality, have produced controversial results that can confuse people when making choices related to their daily diet.”
And my point was that one could use the same logic and similar examples to illustrate that “smoking tobacco is not harmful to everyone”. How useful is that to the discussion?
The reference to the published review article you provided is, on the other hand, much more relevant and useful, so thanks for that.
Maybe I didn’t understand right, but he says no change in the dosing protocol, but he did change brand? That you could be right that you had a decrease from BA which was masked by something different about the Rapa dosing.
Either way, the most surprising thing is that Rapamycin increased your LDL by 60 points?! That’s insane. From what I recall of human studies, that’s an outlier for sure. For me, Rapa (only at 2mg/week) has had no effect on my lipids that I can tell.
Agreed!
That’s awesome. 60mg/dl is a great target when you already have a strong baseline. I had, for some reason, thought you were much younger based on your writing style!. (Take that as a compliment, haha!)
Haha, biology is a big old mess! Probably why I find it so fun and interesting. Measure the same thing multiple times, different times of day, different days, different machines etc and you’ll get different results. Part biological, part analytical.
It’s funny if you really look at research data where you’d expect a pretty consistent response. For example, if you lift weights you’ll gain muscle and get stronger, right? That should be a universally conserved response. However, in actual trials, some people gained no muscle or strength, while others pile on crazy amounts of both. Or you’d think that aerobic training would reliably increase VO2max. Nope - it does on average, but some participants actually reduced VO2max.
Now imagine the number of influences on our circulating cholesterol levels, adding medications etc!
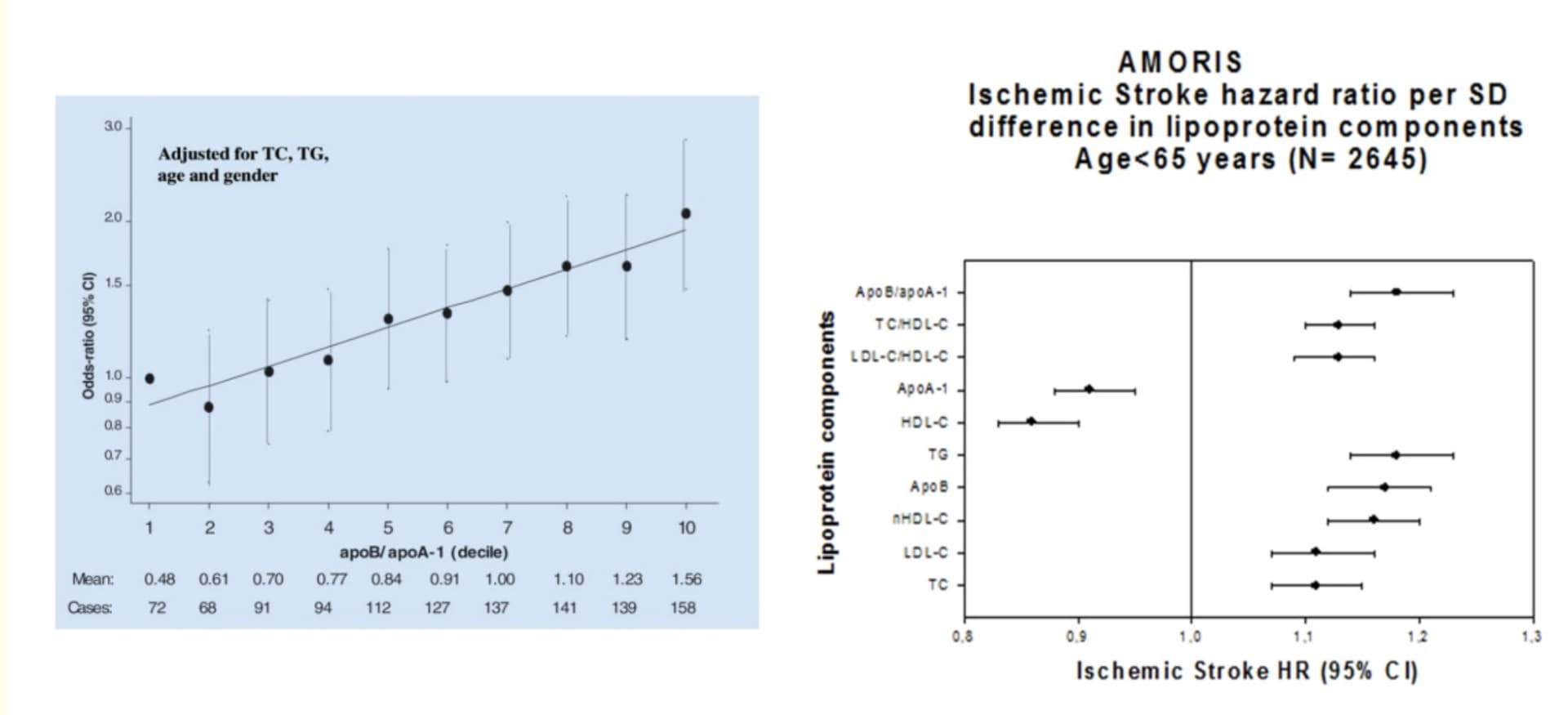
I’m curious - lots of very well researched people here on CVD and cholesterol why the focus on single measure rather than ratios - as my understanding is that ratios are better at predicting CVD or MACE than single measures like LDL-C
You echo my thoughts entirely. I’d love to see more mendelian randomization studies on both psk9 and HMGCR (Statin). The UK biobank data should allow a very clear insight into both ACM and specific diseases.
The research i have seen is inadequate in many ways but does throw up worrying signals for Parkinson’s (Psk9) and cognition (HMGCR).
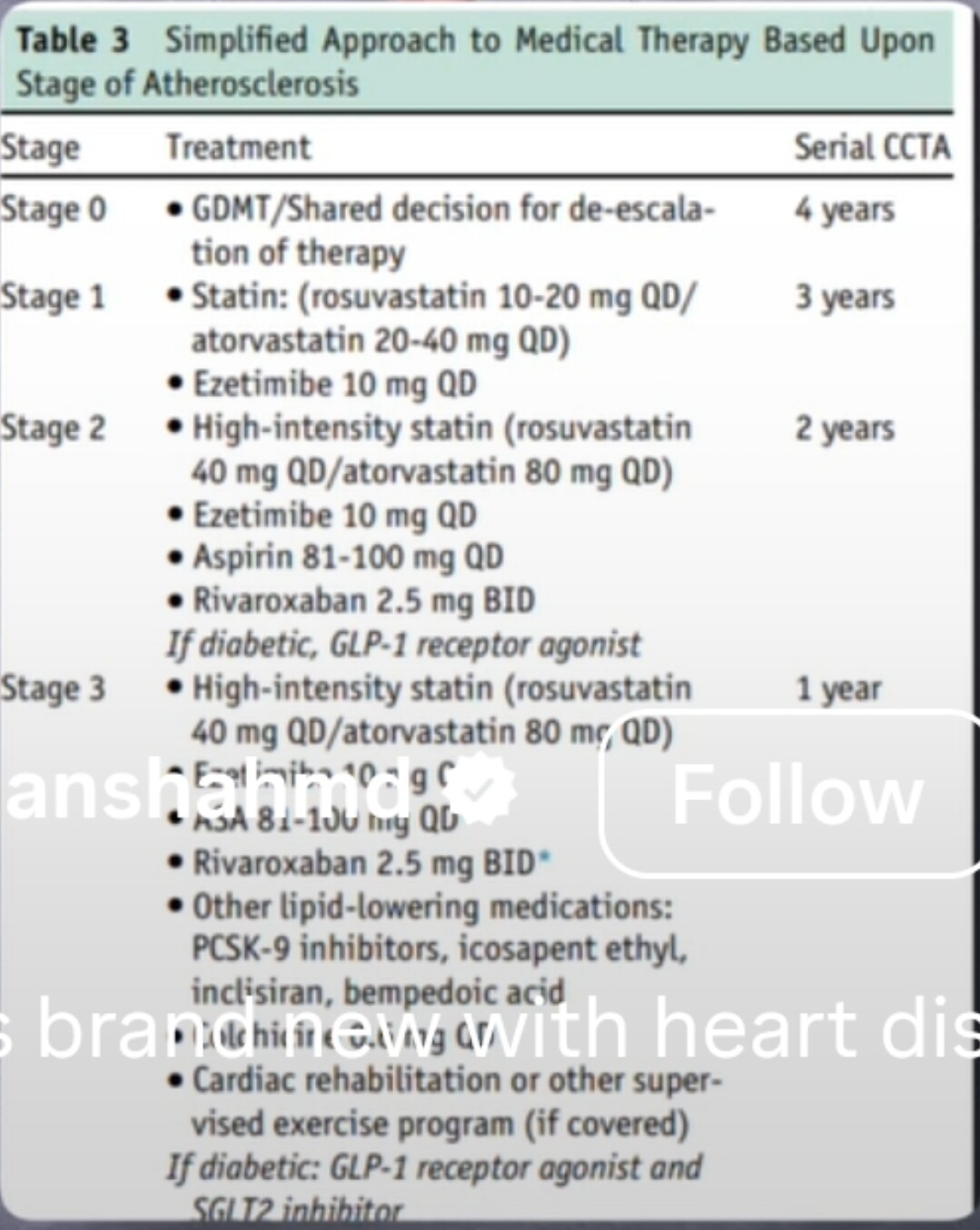
Here’s a recent (April 2025) publication of interest to those of us who have Coronary Artery Calcification and want to prevent it from worsening. The background for me is that I had elevated lipids, low HDL and still have relatively high Lp(a) - 160nmol/L ish. Both parents deceased at age 60 via MIs. I’m now 74yo and fortunately still asymptomatic. My lipid numbers are much improved (70) on max dose Rosuvastatin (which I fortunately tollerate well) + Ezitimibe. I’ve had a series of 3 CAC scans at 2 year intervals with numbers in the sub 300 area reasonably stable since starting PM melatonin 6 years ago. Initially 5mg qhs but i’ve increased that to 120mg qhs for its anticancer and anti-inflammatory properties. My hsCRP is < 1. Maybe it’s the melatonin, maybe it’s the Rosuvastatin. Anyway… for your consideration.
Yes, I do take Rapamycin 5mg qwk with rest periods at intervals. Other medications include Metformin 500mg tid x 2 years ( HbAic is 5.7, same as before starting Metformin) , Doxycyline 5omg qd, Tadalafil 5mg qd (BPH), ASA 81 mg qd x many years, as well as Vitamin C 6 gm/d and Lysine 3gm/d in addition to tocotrienols, Vitamin D 5000iU and a host of other supplements. The above are of course motivated by M Blagosklonny, Linus Pauling, Dr Green and others. So as you speculate I can’t be sure my CAC stability is because of the melatonin, but the article suggests that it may be helping. Just for completeness, I exercise (aerobic + strength), sleep 8 hours per night, and eat a near Vegan diet. I could do with a little more social interaction, but there’s always something to be improved on.
“Kashan University of Medical Sciences, Kashan, Iran” + Mechanistic paper => Might go to the trash (that being said I take melatonin, but not sure this paper is convincing)
If you don’t mind, how much are you taking, and how long have you been taking. Also are there any effects you can report? I ask, because I’m thinking about it, but I have RLS, so I am worried about supplementing with melatonin. Also, off the top of your head, if you supplement, what happens with endogenous melatonin production, does it stop? If it stops, can it resume, or ist it like TRT? Thanks!
I’ve just started testing melatonin. 5 mg IR 1h before bed. 5 mg if I wake up during the night. Better sleep. Unexpectedly stronger morning érections I don’t think trials found an impact on endogenous MLT production. But we don’t have long-term data. When I stop it I’m fine.
About my sleep: when I was taking melatonin, 3 - 5 mg my sleep was ok (7-8 h), when I stopped it’s still ok but the deep sleep stage increased. Coincidence?