Epidemiological studies are actually good but RCT’s and MR fill in the gaps and takes care of residual confounding, so they supersede them if they are in contradiction.
2 Likes
Maybe I’m too dumb but I don’t “get” that site. A lot of the “arguments” with good “banger ratings” (I assume that means truthfulness) are weird, nonsensical or false?
I like your numbers. This is a great succinct summary of a lot of studies!
The only thing I’d add is that if anyone has diabetes or pre-diabetes, the best thing for avoiding cvd and all cause mortality is to reverse it. By all means squash down LDL-C in the meantime - but getting HbA1c down should be their highest priority.
2 Likes
As promised I’m posting results of the n=1 experiment wrt. lipid medication. No changes in diet or exercise or other lifestyle factors, sleep, level of stress insofar as I can tell (low), supplements. One change in medication: went from empagliflozin 12.5mg/day to 25mg/day and an additional change - sirolimus: same dose 6mg/1-week, but this time it was only 3 weeks of the Zydus brand vs 11+ weeks of the Eris brand, and the Zydus came after a 7 week break from rapa.
Pitavastatin 4mg/day alone vs pitavastatin 4mg/day + bempedoic acid 180mg/day.
Pita alone - 5 months; Pita + BA - 39 days.
Legend: Pita alone - PA; Pita + BA - P+BA.
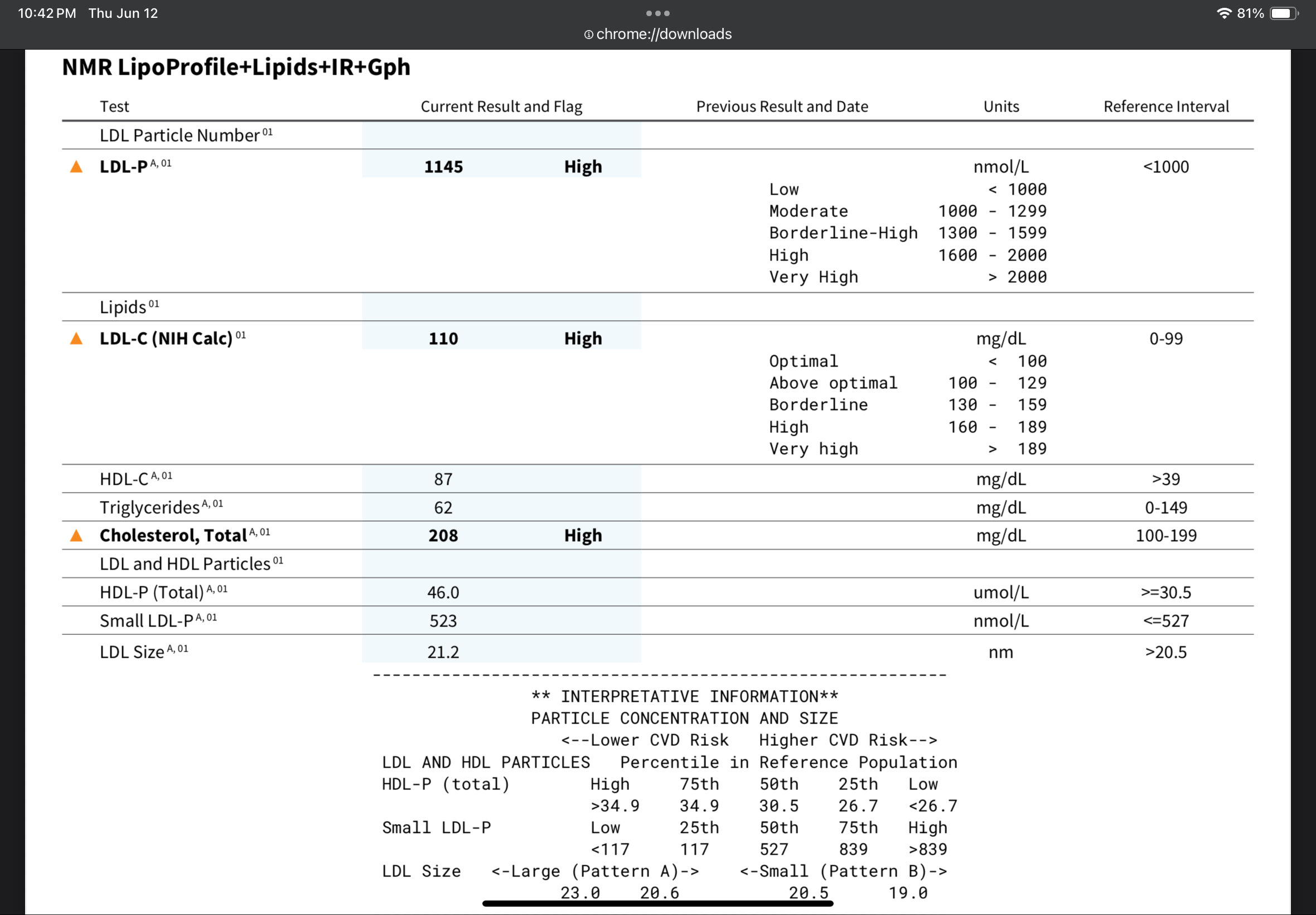
Total Cholesterol: PA - 228 mg/dL ; P+BA - 208 mg/dL
LDL-C Calc: PA - 123 ; P+BA 110
Trig: PA - 93 mg/dL ; P+BA - 62 mg/dL
HDL: PA - 89 ; P+BA - 87
However, several biomarkers went in the wrong direction, some to a worrying degree (worst I ever had!), and a couple went in a better direction. Short of it: better direction - glucose and insulin (I didn’t do HbA1c because it had not been 3 months since my last test). Worse direction: hsCRP, homocystein, RDW, neutrophils, lymphs, sodium, chloride, and so on. Current is P+BA and previous is PA.
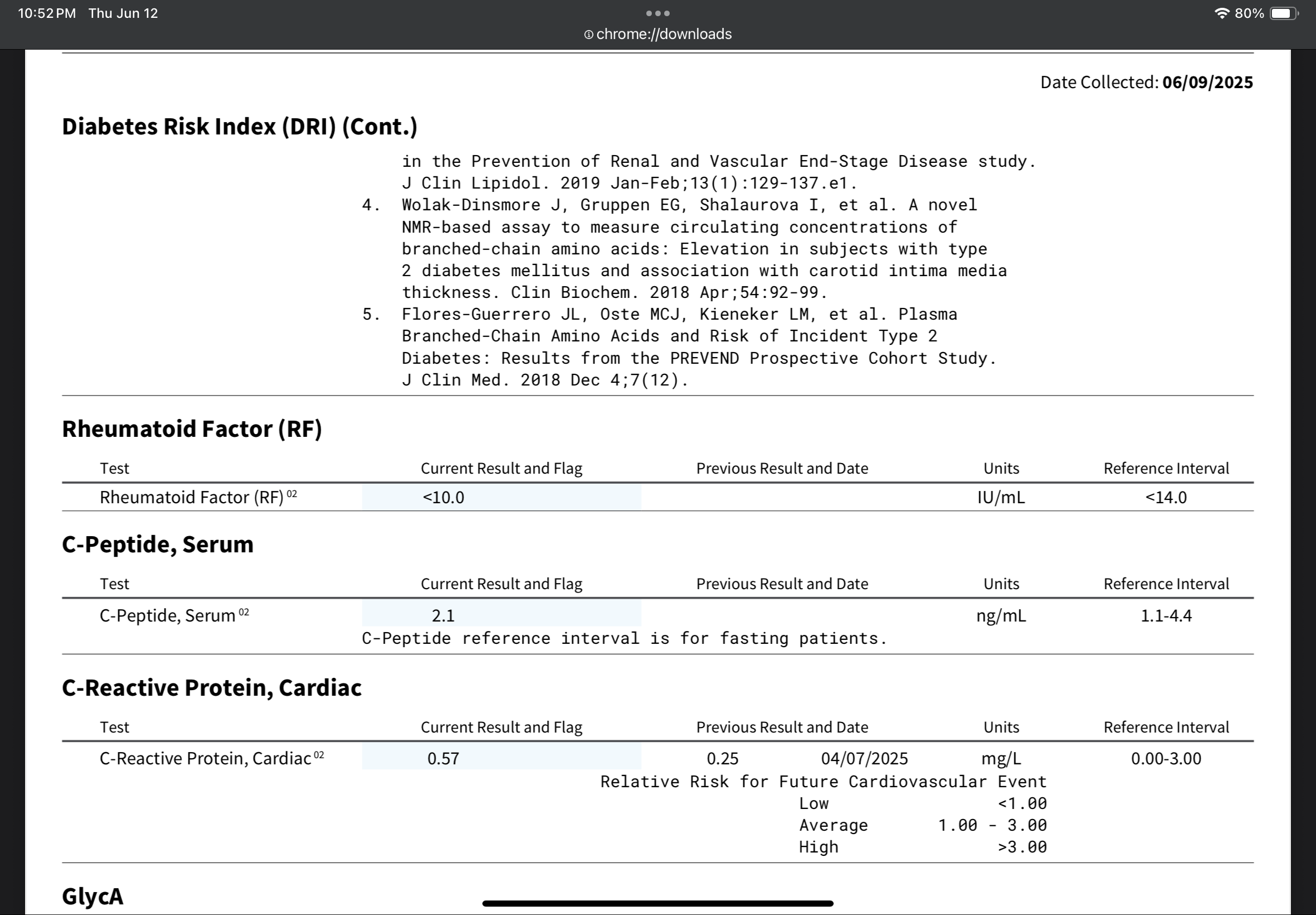
hsCRP: PA - 0.25 mg/L ; P+BA - 0.57 mg/L
homocysteine: PA - 7 umol/L ; P+BA - 10.8 umol/L
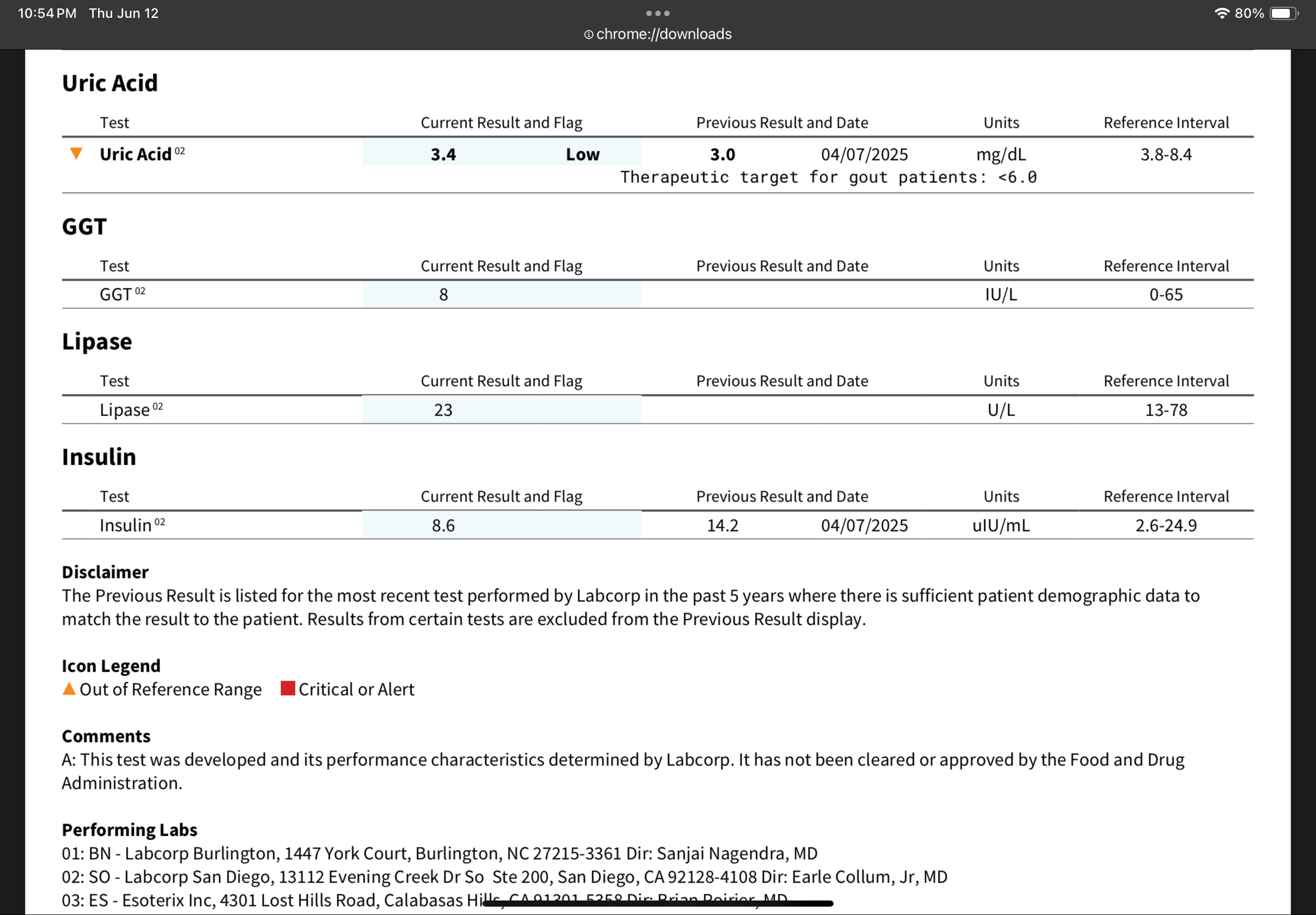
uric acid: PA - 3.0 mg/dL ; P+BA - 3.4 mg/dL
insulin: PA - 14.2 uIU/mL ; P+BA 8.6 uIU/mL
sirolimus: PA - 5.6 ng/mL ; P+BA - 4.4 ng/mL [note: both tests were performed 49-51 hours after last dose of rapamycin, taken on an empty stomach, same protocol]
So I don’t know what to make of this. Lipids in general seem to be going in a better direction, but not by a ton on the addition of BA, liver enzymes also largely better, and the uric acid went up by 0.4 from 3.0 to 3.4. So the liver, uric acid seem to be OK with BA. Meanwhile why has my hsCRP rocketed from 0.25 to 0.57 - the highest I’ve ever had my hsCRP measured was 0.4 - so 0.57 is shocking, but BA is supposed to lower the hsCRP, so who knows. My RDW went from a nice 11.8 to a catastrophic 13.4 - insane, I’ve never had it so high, ever, worst was like 12.x something. The glucose I also don’t know what to make of, because the only change was going from 12.5mg/day to 25mg/day of empagliflozin which seems a rather dramatic change for such an insignificant factor as a doubling of empagliflozin, which is not a result I’d expect based on the empagliflozin literature; also, the 12.5mg/day dose was measured in the PA test after 4 months, whereas the BA test with the 25mg/day was after 39 days on that dose. Plus the insulin went way lower, and empagliflozin is not an insulin sensitizer. The sodium and chloride is worrisome, but perhaps I was somewhat dehydrated as I had no food or liquids for 18 hours, but my blood tests are all taken at least 14 hours of fasting with no liquids - FWIW, I don’t add salt to my food, don’t eat much in the way of processed food, and empagliflozin is not supposed to retain sodium if anything the opposite. So who knows.
The sirolimus is interesting insofar as there are two factors here. No change in the dosing protocol, but first, the PA test was with Eris BioCon, whereas the P+BA was with the Zydus brand; second, the Eris was after 11 weeks, wheras the Zydus was after a 7 week break from rapamycin (due to surgery) and after 3 weeks of taking Zydus. Also a rather dramatic difference, going from 5.6 to 4.4. Possibly, rapamycin accumulates with time for me, or perhaps some other reason. I am going back to the Eris/BioCon brand at the same dose protocol and will retest the sirolimus, though not the next test as I wan to first test my sirolimus level on the last day before the next dose, to see what my lowest level is before the next dose 24 hours later. But then in the test after that test, I’ll go back to testing the 50 hour level, at which point it should again be 11 weeks of the Eris/BioCon brand so we’ll see if it’s something random in my body or a consistent effect.
The bottom line in all of this, is that you should test often - because your test results might be a one off, and you don’t want to make big interventions based on unreliable one off results. This is why I’m testing repeatedly, even though it’s $500+ every time with so many tests. I figure after 8-10 of these, I’ll have more reliable results… although if spread over a year, I must account for the effect of becoming increasingly older ![]() .
.
Next test will be pitavastatin 4mg/day + ezetimibe 10mg/day. This time I’ll be on the ezetimibe for 50 days, so a little longer, to give my body a chance to wash out the BA. I’ll post the results again - I’ll be testing in early August.
8 Likes
Please report prices paid for individual tests.
Unless there’s a raft of tests you didn’t list here, I don’t see how you could spend this much.
1 Like
At 6mg/week that’s quite possible and common. You need to test your rapamycin levels at 48h and 96h to check the half life.
1 Like
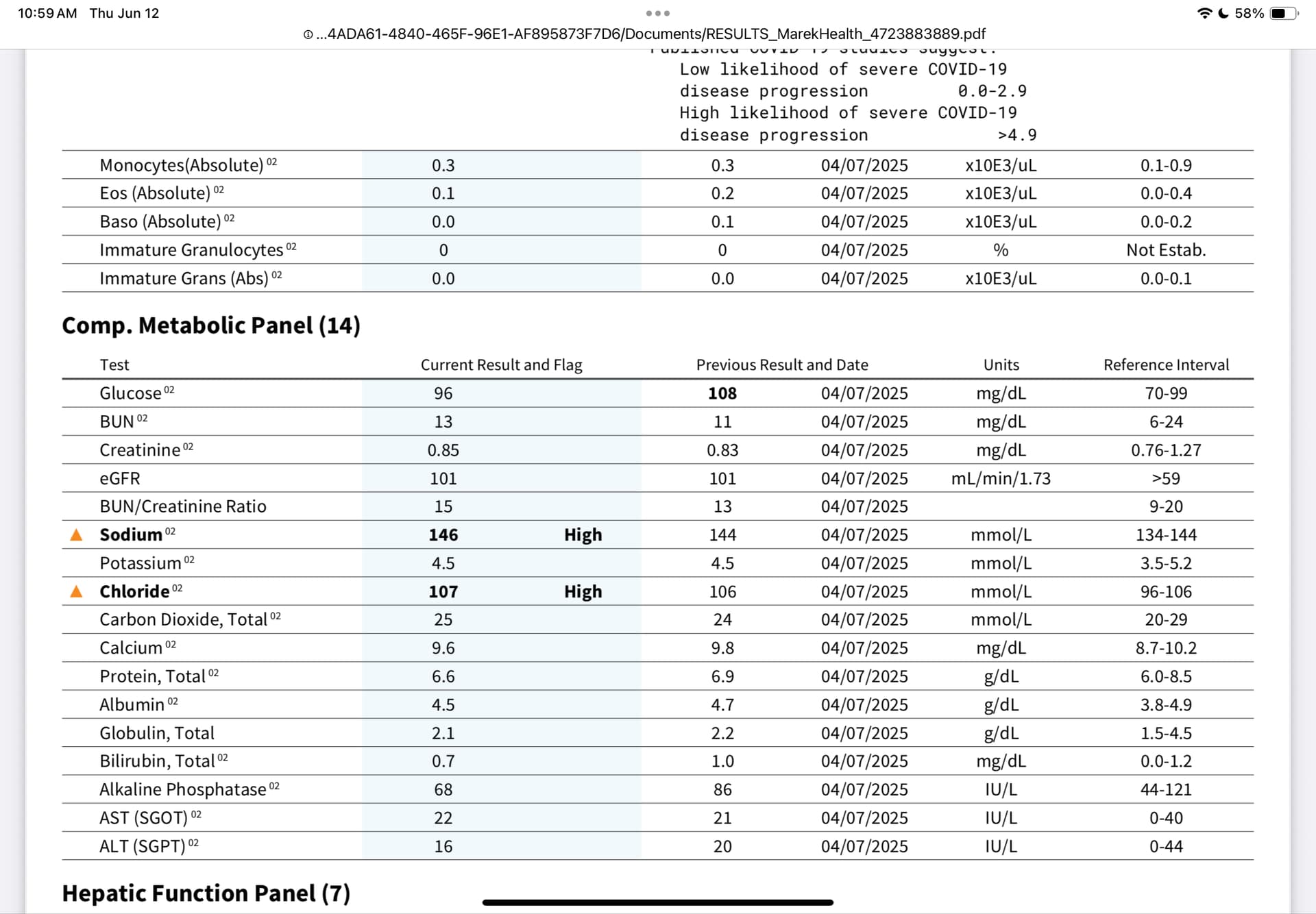
Yes, there is a bunch I did not list in that post.
First test with pitavastatin alone - came to $519, ordered from Marek Health.
Second test:
I will go to the Marek Health website to get the test prices later today and post them here (you can also go to the website and check them).
I did not publish many tests in the other post as I saw no relevance (lead levels in blood etc.). I also checked the prices against ownyourlabs.com and found Marek Health to be the lowest. You are welcome to doublecheck the prices on both websites.
Lead, blood - $20
Sirolimus, blood - $65
Uric Acid - $10
Hepatic Function Panel - $6
IGF-1 - $45
Sex Horm Binding Glob, serum - $40
Insulin - $15
Testosterone, Free and Total - $34
Hemoglobin A1c - $9
CBC with diff, platelet, NLR - $10
Lipid Panel with HDL/LDL ratio - $10
Apolipoprotein B - $17
Lipoprotein A - $35
C reactive protein - $23
Lp-PLA2 Activity - $50
Homocysteine - $65
OmegaCheck - NO LONGER PROVIDED BY MAREK HEALTH SO NO PRICE CURRENTLY
Comprehensive metabolic panel - $10
There’s also some venipuncture charge.
The total came to $519. Unfortunately I don’t remember the omegacheck or venipuncture charges, but it came to $519:
Have I been transparent enough to your satsisfaction or have I fallen short?
The idea was to find a way to save you some money. You could have just said: ‘Yep, there’s a ton of tests I didn’t list here.’ and left it at that. But you being you…
You may want to consider signing up for a Fitomics membership.
Cost at Marek for homocysteine -
Cost at Fitomics -
$40 cheaper than Marek. Right there, you can cover the $30 signup fee and save $10. I’m not going through all your tests, but at worst they likely match Marek, and in most cases, somewhat to substantially cheaper. Unfortunately, you can’t see the price list until after you sign up. But here’s one example from my orders -
Marek offers 10% discount codes (I hope you’ve been exploiting this!). They’re always changing, can be used only once.
At Fitomics, code ‘discordlabs’ always gets you 5% off. And there’s no blood draw fee.
Furthermore, you can sign up for one month, make multiple orders covering several months of tests, and then cancel at the end of the month. Re-enroll in six months, repeat.
Might not be as comprehensive as Marek. I’m told if they don’t offer a test, you can request it to be added. Haven’t tried.
The pricing here may not last, so make hay while the sun shines.
Note: This is for LabCorp tests. Fitomics also has a Quest shop, but it’s retail pricing.
Also: When you create a Fitomics account, ensure you have an address shown in the account information. Otherwise, they will generate an order with no address, and it will not be picked up by patient.labcorp.com. You can get the address added at the labcorp visit, if you forget.
9 Likes
Thank you for that tip. One limitation sometimes is a lack of blood sirolimus. But, genuinly thank you, I have not been especially smart money-wise, haven’t seen any Marek coupons or discounts. Some tests are more expensive, like IL-6, almost $200. I will look into this.
1 Like
You buy IL-6 here:
Sirolimus test can be found cheaper than Marek, it’s been discussed elsewere, I lost track.
You can walk into LabCorp with multiple orders from different vendors, I do it all the time. I tend to put all the ones that can be done overnight in one order, others that take longer in another order(s). Because I dislike waiting for results.
5 Likes
I got my sirolimus tests with gethealthspan.com
If I recall, it was $25 and you go to labcorp
4 Likes
Thank you guys for all the valuable money saving tips. Lacking the “thrifty” gene, I have been quite negligent financially, and tend to take the “easy” way out and just pay more (for drugs, tests, treatments etc.). I will try to do better.
2 Likes
I also like the getHealthSpan.com labs packages. They have great options from $40 to $350 that cover a lot more tests than what you are testing. Check them out to save money and get more comprehensive tests!
3 Likes
This might be relevant if eggs vs health were an area of unexplored research and anecdotes were being used to generate new hypotheses. It’s not.
You were attempting to use anecdotes from a grand total of 2 persons as a reason to refute published studies in thousands of actual research subjects.
2 Likes
Based on this, I’d say BA isn’t working for you at all. All of those are within the margin of error and normal variability IMO. Like, you could test a Monday and Tuesday and get LDL-C of 123 and 110, and I wouldn’t value the -13mg/dl change at all.
Ezetimibe was super effective for me.
As for all the other changes, they do look worse, but there’s always natural variation. Like, you might have picked up a slight infection or something. that you didn’t notice.
But, based on the big jump in RDW% (which I feel is like a signature of Rapamycin activity), I would guess the change of Rapa brand might be the issue. Even then, the absorption etc can be affected by what you ate around the dosing or after the dosing and all sorts of other variables. Your MCV came back super consistent, so if the mean is the same and RDW% is larger, that would have to mean you have equally greater populations of both smaller and larger cells. It makes me wonder how well calibrated their machine and gating parameters are. This is biology, not an exact science, hehe.
I would say, bearing in mind that this is the cardiovascular health thread… you’re looking at rapamycin levels and worrying about RDW%, while also sitting there right now with an LDL-C of more than 100mg/dl which is known to be sufficient to generate plaque. I’m not trying to attack or criticise or in any way demean your testing here, but just be careful not to get lost in the details and miss the bigger picture. If I objectively look at this set of results, the only thing I’d say you can do something about is the LDL-C.
2 Likes
The issue is that he changed his Rapamycin dose (which negatively affects lipids) and added Bempedoic Acid (which positively affects lipids). Rapamycin increased my LDL by 60 pts. So , if the same thing happened to him, Bempedoic Acid could have reduced his LDL by up to 73 points which would be phenomenal.
That’s why you don’t change two variables at the same time. The only way to know for sure is to change one variable back and look at the difference.
1 Like
Thank you. Yes, the LDL is in question here. I am not super surprised by these results. While BA works upstream from a statin, it’s in roughly the same biochemical pathway. Given that I was on the max pitavastatin dose, I wasn’t expecting much more from the addition of BA, it was more like going from a moderate intensity statin (pita alone), to a high intensity one, and as we know, you get the vast majority of the LDL lowering from the initial dose of the statin and proportionally much less going up in dose. Moderate intensity statin + BA = likely underwhelming additional lipid lowering.
Meawhile ezetimibe works on a completely different pathway, and the literature seems to suggest it’s complementary to a statin. I expect a much stronger effect, especially if I’m a high absorber of bile cholesterol.
And because with biology there are always surprises and unexpected effects, I intend to also test the P+EZ+BA combo. If I can reach my lipid goals with P+EZ alone, fantastic, I’m happy to drop BA, as long as my other markers are not somehow affected negatively. My goal for LDL, is dropping below 60 mg/dL, so even if it’s just 55 mg/dL, I’d be satisfied, considering that my CAC at 65 was zero. I intend to do another CAC in 2-3 years, just to keep tabs on what is happening with my vasculature/atherosclerosis.
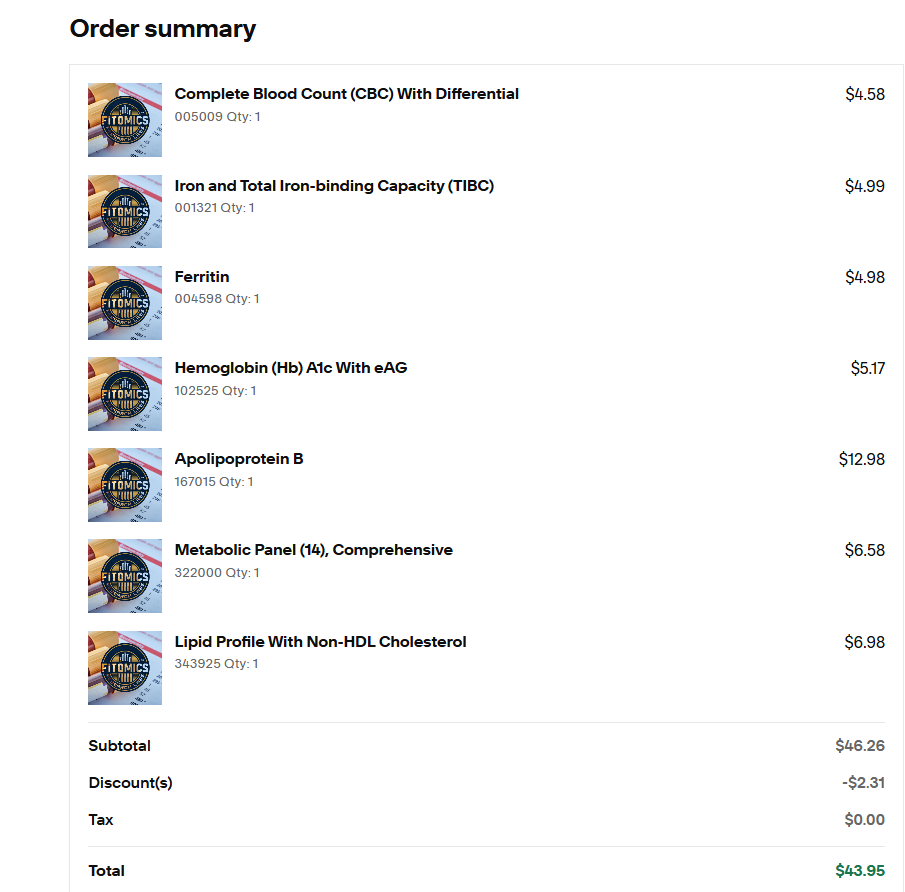
FWIW, here is a bit more data from my test:
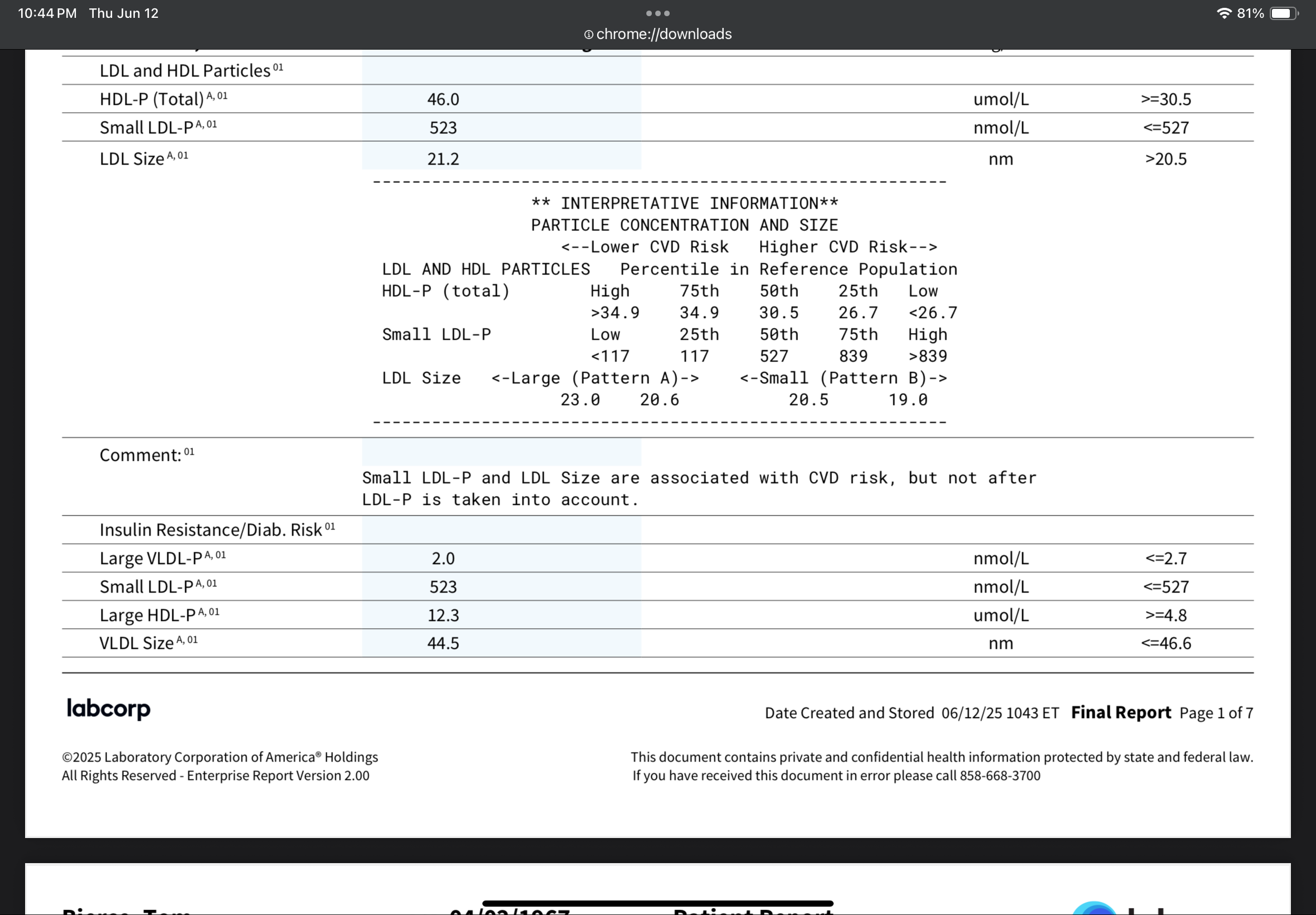
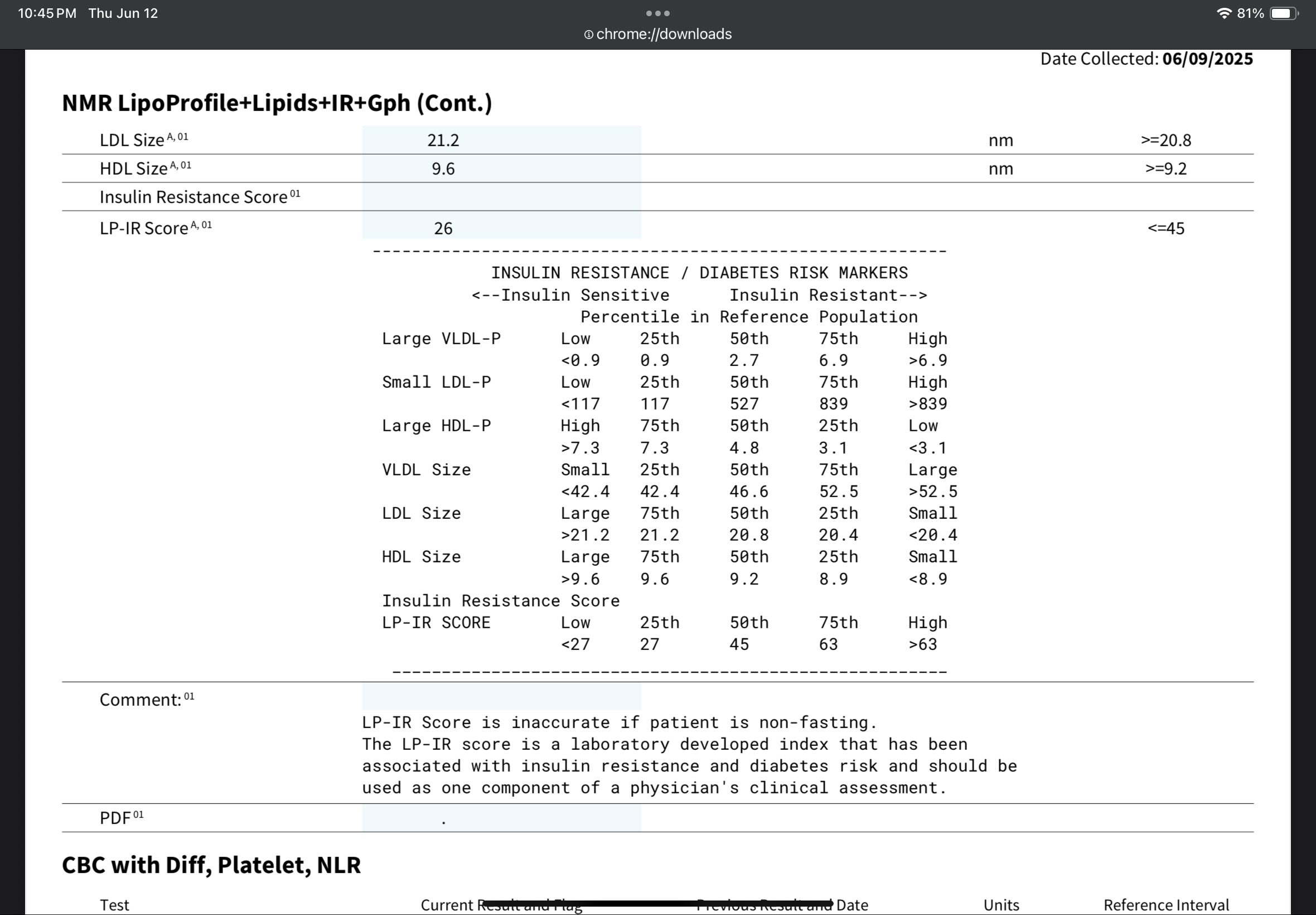
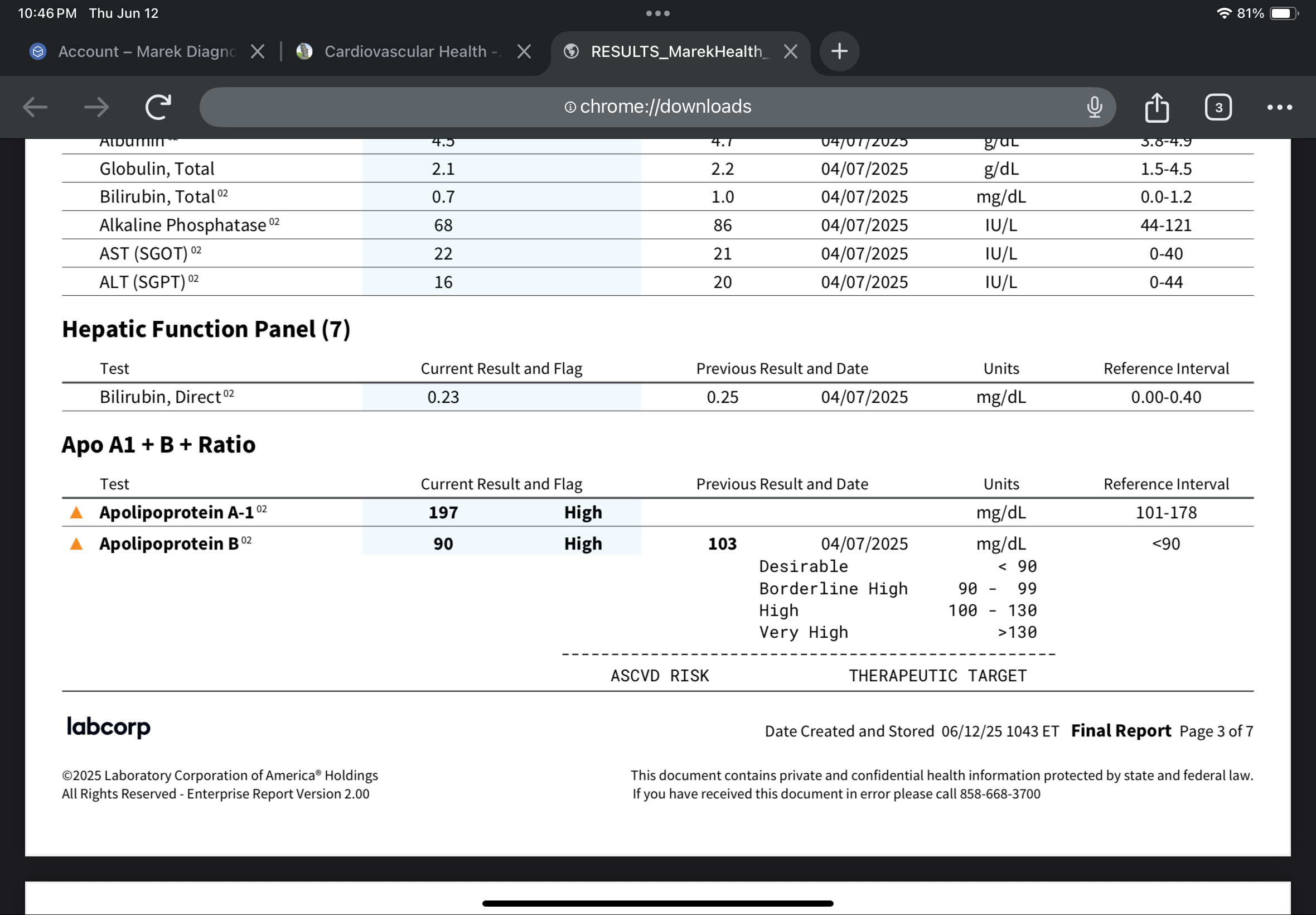
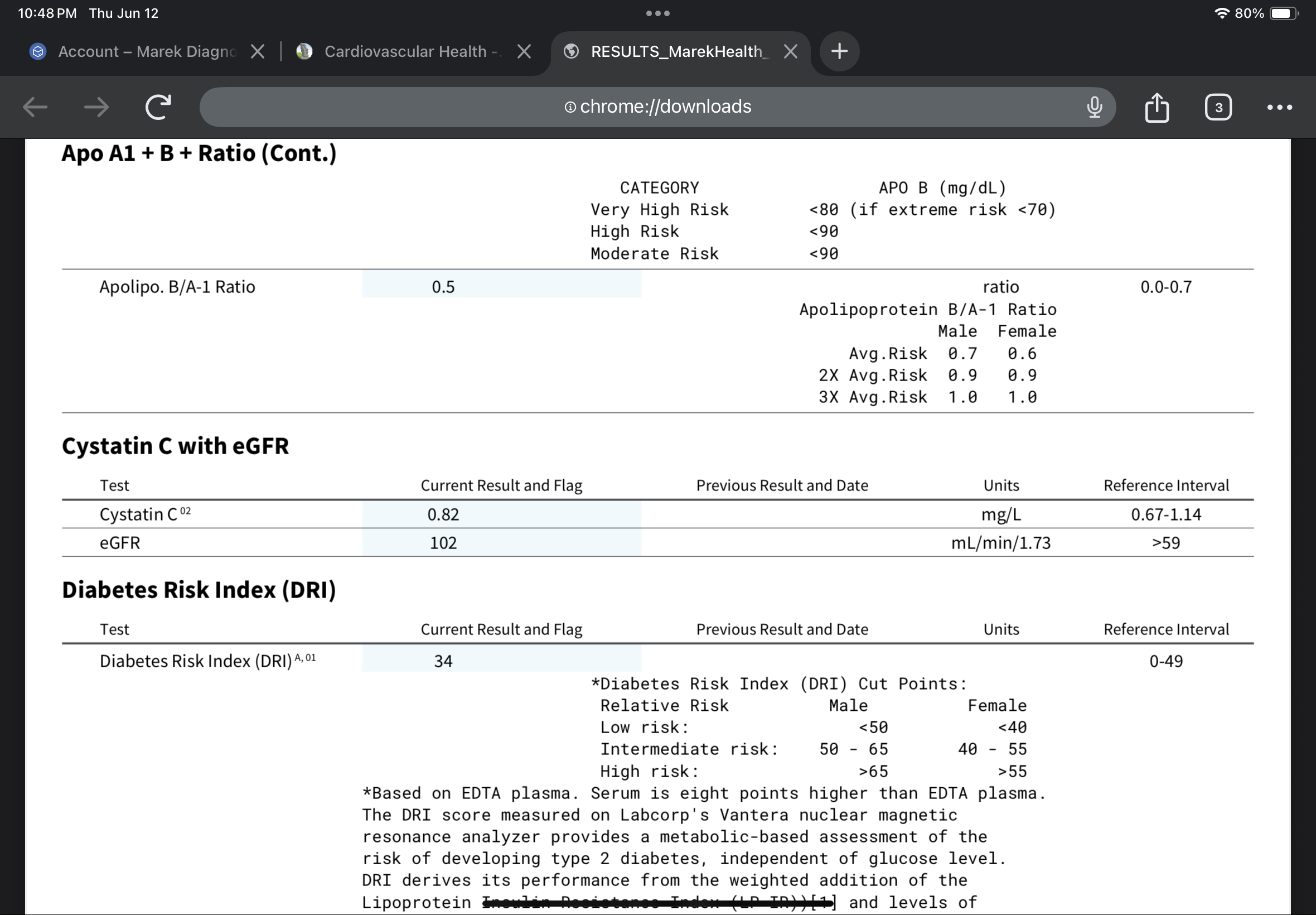
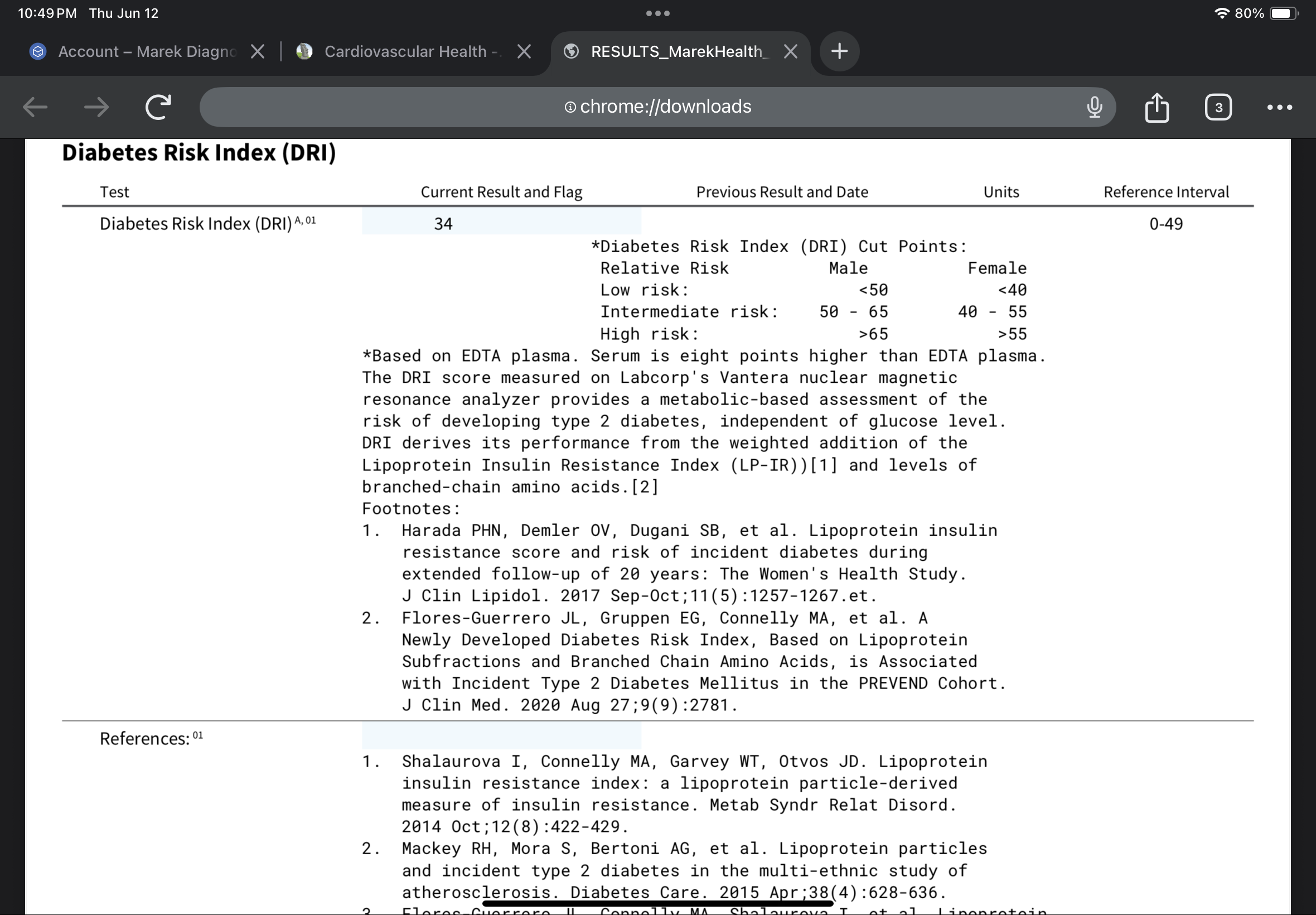
I thought the study references were pretty interesting, which is why I included them.
2 Likes
@CronosTempi I know you are very thoughtful about what you take and you are much more knowledgeable about all the options than I am, but because I know it’s in your budget, is there a reason you are not adding repatha? I don’t tolerate statins and am on it with dramatic results. It seems that might be the one two punch that makes all the difference for you?
@relaxedmeatball I didn’t realize those little moves in lipids might not necessarily be from our medicines… again, I’ve learned something. I’ll have to go back and look at my labs, but if that is the case, BA might, oddly, do zero for me. I’ll continue to take it just because I have it, and seems harmless, and what if it does help, but interesting.
I have no specific objection to PCSK9i, but before I take any drug, I try to study it as much as possible. I do not feel that I have enough of a grasp on the very long term effects of these inhibitors apart from the LDL lowering effects. In populations of the naturally inhibited, what is the prevalence of centenarians? I guess I’m a lot slower than most - especially on this site - in deciding to take any drug, supplement or intervention. I need to know a lot more about these inhibitors before taking the plunge. If pitavastatin plus ezetimibe or BA can get me to my LDL goal, I feel no urgency to try a PCSK9i. I’ll keep studying them for now.
In your case, with an urgent and compelling need for drastic lowering of lipids (in contrast, my CAC score was zero at age 65), and statin intolerance (not my case), a PCSK9i is highly indicated (assuming you are not intolerant to it). Our cases are very different, so my decision tree here is not instructive. If I were in your shoes I would absolutely take it. I think you are doing the right thing.
Chinese paper, but from good institutions.
Exploring the Pleiotropy of PCSK9: A Wide Range of Influences from Lipid Regulation to Extrahepatic Function
2 Likes
I knew you’ve have a very well thought out reason ![]()
And yeah, I’d eat styrofoam if it were proven to help!
And yes, I keep toying with the idea of statins for their calcification properties… I’m jealous of those who can take advantage