A disturbing must-see video for statin users such as myself.
# Statins Slash GLP-1 Levels: Human Controlled Trial

A disturbing must-see video for statin users such as myself.
# Statins Slash GLP-1 Levels: Human Controlled Trial
The same people who take this guy seriously also believe that cancer has been cured every time a popsci article says that X cures cancer because it worked in a petri dish.
It’s a real issue. Obicetrapib + ezetimibe will solve that problem.
Please - if anyone is posting a video now, include an AI summary (from here or other… Krisp | Free Youtube Video Summarizer with AI
Introduction to Statins and GLP-1 Levels
Lack of Awareness in the Medical Community
Study Overview and Key Findings
Mechanism of Action: Statins and Gut Microbiome
Animal Model Confirmation
Human Pilot Trial with UDCA
Broader Implications and Call to Action
Conclusion and Recommendations
He has credentials: a PhD in Human Metabolism at Oxford and an MD from Harvard.
I will take his opinion any day over yours. What are your credentials?
At no point did he suggest that people should stop taking statins.
Your main contribution seems to be trolling.
I take statins and rapamycin, both of which raise my A1C, and I can’t tolerate metformin.
So, yes, I am going to take TUDCA for at least 30 days and monitor what it does to my fasting glucose levels and A1C.
Can we move these discussions somewhere else than the flozin thread? We have a UDCA & TUDCA thread by the way: UDCA (ursodiol) / TUDCA for healthspan and lifespan?
Every single statin denialist I’ve interacted with has also been an LDL cholesterol denialist, without fail. Really remarkable.
I might change my statin (currently atorvastatin) to a less glucose/insulin impacting version. My fasting blood glucose levels have been hovering around the 95 to 105 level and I’m wondering if changing statin might lower these…
ChatGPT Query: are some statins better than others in terms of contributing to insulin resistance, increasing the risk of type 2 diabetes, and significantly lowering GLP-1 levels in human?
Yes — different statins vary in how much they affect insulin resistance, type 2 diabetes (T2D) risk, and GLP-1 levels. Here’s a breakdown based on the best available clinical and mechanistic data:
Higher risk (more likely to impair insulin sensitivity and increase T2D incidence):
Lower risk (neutral or sometimes beneficial for insulin sensitivity):
Evidence (still limited, mostly small human studies + animal work):
Statins impair glucose metabolism through:
Potency, dose, and lipophilicity matter:
If it’s diabetes risk you care about, atorvastatin is better than rosuvastatin. Just like with other side effects, testing around.
Use CGM’s as well before and after swapping. Do a OGTT before and after. Peter Attia knows a lot about this.
My LDL-C is extremely low right now - around 46 I think at last measure, so I’m thinking of moving to pravastatin to see how it impacts my fasting glucose levels. I don’t worry if my LDL-C / APO-B goes up a few points.
That’s what Brad Stanfield did. Not something I think is future proof. I’m suspecting we will learn that lower is better for sure. It’s not going in the other direction.
Fasting glucose is not that informative on its own, that I know. But if you can keep your glucose lower while apoB the same that’s better of course.
It’s an interesting question… which is more damaging to the body, 5 or 10 points on LDL-C or fasting Blood glucose measurements? I don’t think we have an answer yet do we?
I’ve not really heard people talk about fasting glucose in isolation, it’s always relative to insulin levels taken at the same time for HOMA-IR calculation, and even better is OGTT according to Peter Attia. Of course there are association studies of the optimal levels but it might be a separate issue.
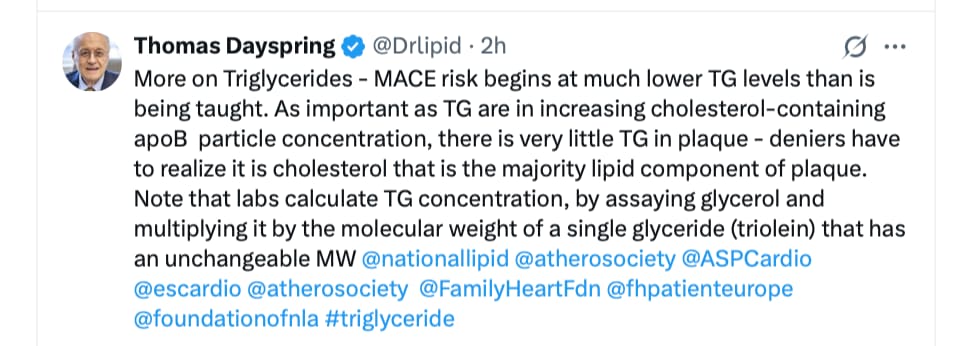
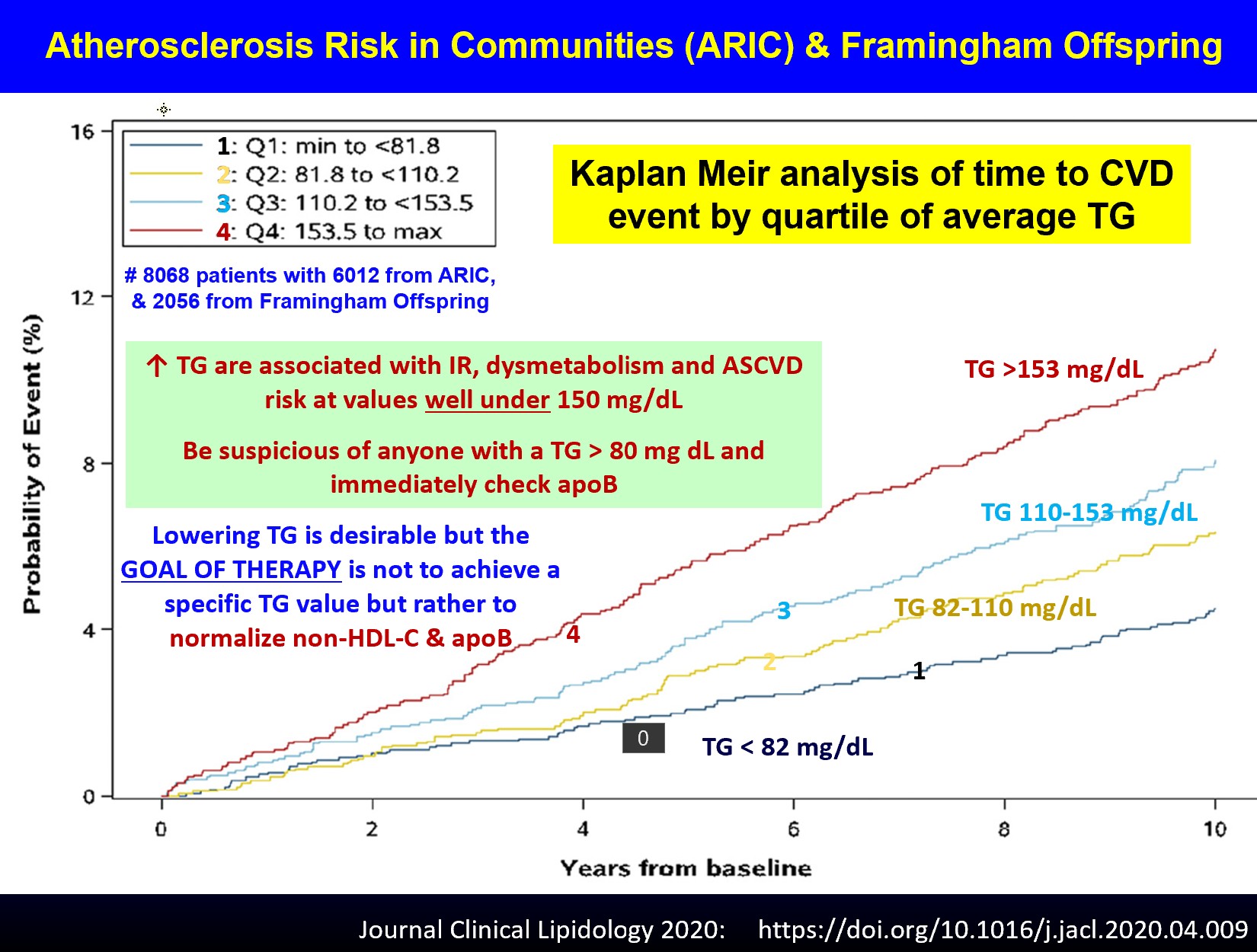
As he wrote, it’s the non-HDL-C and apoB that matters, not lowering to a specific triglyceride level (which is e.g a marker of insulin resistance/diabetes).
AI answer:
An isolated +10 mg/dL rise in apolipoprotein B (apoB) with a simultaneous –10 mg/dL drop in fasting glucose is generally more harmful than the opposite change (‑10 mg/dL apoB, +10 mg/dL glucose), especially when the glucose change stays within the normal range.
Why a 10‑mg/dL increase in apoB carries more risk
Factor What the number means Typical risk per 10‑mg/dL change (approx.) Why it matters apoB Each 10 mg/dL rise reflects ≈10 % more circulating atherogenic particles (VLDL‑apoB, LDL‑apoB, Lp(a)‑apoB). ≈6–9 % higher risk of major atherosclerotic cardiovascular disease (ASCVD) events in prospective cohorts, independent of LDL‑C. apoB is the direct count of atherogenic lipoprotein particles; every extra particle can enter the arterial wall, become oxidized, and trigger plaque formation. Fasting glucose A 10‑mg/dL rise is ≈0.55 mmol/L. In a person whose glucose is already in the normal range (e.g., 85 → 95 mg/dL) this is still well below the diabetic threshold (126 mg/dL). ≈1–2 % higher risk of ASCVD (if glucose stays <100 mg/dL) and very modest impact on microvascular risk. Glucose‑related damage is largely a function of chronic hyperglycemia (≥126 mg/dL fasting) or sustained elevations that raise HbA1c >6.5 %. A single 10‑mg/dL bump rarely pushes a normoglycemic person into that high‑risk zone.
It makes sense, as long as you’re not diabetic or becoming so and harming the arteries with excess glucose, it’s better.
The FDA approved Repatha for primary prevention. https://www.medpagetoday.com/cardiology/dyslipidemia/117148
Unfortunately there are always tradeoffs.
“Compared with baseline values, patients treated with atorvastatin had no change in atheroma burden, whereas patients treated with pravastatin showed progression of coronary atherosclerosis.”
Of course this paper’s subjects had a higher BMI, and the dosages were not adjusted so it’s not exactly apples to apples.
As I previously posted, I will give TUDCA a trial.
That is a really interesting question!
This suggests there are threshold effects for hba1c
" There was a non-linear relationship between mean HbA1c during follow-up and the risks of macrovascular events, microvascular events and death. Within the range of HbA1c studied (5.5–10.5%), there was evidence of ‘thresholds’, such that below HbA1c levels of 7.0% for macrovascular events and death, and 6.5% for microvascular events, there was no significant change in risks (all p > 0.8). Above these thresholds, the risks increased significantly: every 1% higher HbA1c level was associated with a 38% higher risk of a macrovascular event, a 40% higher risk of a microvascular event and a 38% higher risk of death (all p < 0.0001)."
Association of HbA1c levels with vascular complications and death in patients with type 2 diabetes: evidence of glycaemic thresholds | Diabetologia)
I guess so. End of the day, we are not chimps or lions and I just don’t think we should be setting them up as any sort of comparison. Lion diets consist entirely of red meat and they don’t get heart attacks. Weirdly the horse has high cholesterol, but they are cardiovascularly extremely fit. I think every organism has unique physiology.
Yep, and honestly, I think these lipidologist people are also making a mistake of getting into the weeds on this sort of argument. The whole “appeal to nature” thing is bullshit. I also think that “20-40mg/dl is normal” is a stupid statement. It’s trying to hijack the natural = best argument. It would simply be better to say 20-40mg/dl is optimal for ASCVD prevention, without trying to make appeals to nature IMO.
The key word here is “potential”. As far as I know, the actual evidence still massively favours using statins. To get excited about changes in GLP-1 or bacterial metabolites is maybe putting the cart in front of the horse. It’s academically interesting but I don’t think it’s worth the “hype”. As @desertshores says, there are always trade-offs. The important thing is overall outcomes. You take a statin to address one thing, which causes something else to change, and then something else (like TUDCA) is taken to address that. But TUDCA itself has drug interactions, so the cycle will never end haha.