Thomas Dayspring have said it’s a surrogate for apoB.
Thomas Dayspring might have said that, but the paper definitely does not. “Adjusting the model for age, sex, LDL-C and ApoB levels demonstrated that the association of LDL-TG with atherosclerosis was independent of these well-known factors [, including ApoB].”
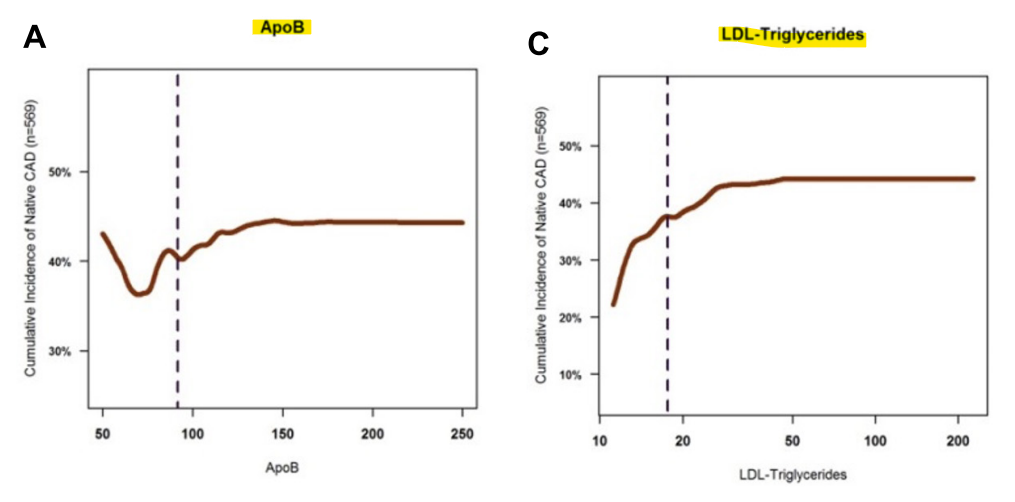
Just look at the chart for the population in the study for ApoB and LDL-TG. You could be patting yourself on the back for having lowered your ApoB < 50 with statins, but your LDL-TG could still be elevated, increasing your CAD risk.
Looks like that study method is B.S. with a B.S graph.
50 apoB doesn’t have the same risk as 120 apoB. Just another fake U-shape curve with residual confounding.
It would be nice if there was a way to get LDL-TG from TG and LDL-C. I couldn’t find any resource online to do that. FWIW, I asked ChatGPT and got the following.
It is not possible to calculate LDL-TG (low-density lipoprotein triglycerides) directly from a standard lipid panel because such panels typically report:
Total cholesterol
High-density lipoprotein (HDL) cholesterol
Triglycerides
LDL cholesterol (calculated or measured)
The triglycerides reported in the standard lipid panel reflect all triglyceride-rich lipoproteins, not specifically those in LDL particles. LDL particles typically contain very little triglyceride, and LDL-TG levels are not routinely measured in standard clinical settings.
Methods to Estimate LDL-TG
To measure or estimate LDL-TG, specialized techniques like ultracentrifugation or nuclear magnetic resonance (NMR) spectroscopy are required. These methods separate LDL from other lipoproteins and allow for direct triglyceride content analysis.
If you’re interested in exploring this, it’s best to consult with a healthcare provider or a lipid specialist to discuss the need for advanced lipid testing.
EDIT: @adssx shares a way to estimate LDL-TG here.
But that’s only the estimated LDL-TG (eLDL-TG). If you want to find your real LDL-TG you need to test it but as you said it’s not commercially available in most labs.
They tend to stick less than small particles but contain more cholesterol so overall the net effect is the same for both types.
Imagine a cal 50 BMG round hitting you once or 9mm bullets hitting you 10 times. In both cases you’d end up dead.
It’s not the impact that matters most of the time, it’s the amount of bullets, so the 10 9mm bullets would be more harmful to the arterial wall in this context… that’s what apoB measures.
Not sure about LDL particle sizes. LDL-TG is a component of LDL, so maybe LDL size doesn’t matter as much?
Using your lipid values to estimate LDL-TG, I get 31 mg/dL. Per the paper, ideally you would want this below 20. In your case, the main target would be lowering triglycerides. But who knows, the estimate only has a R2 of 60%, so there’s a lot of room for error.
Statin update. It seems I am even intolerant to 5 mg of Atorvastatin. I switched to a Monday-Wednesday-Friday night dosing schedule and the muscle spasms stopped, but I still experience muscle weakness in my calves and thighs on Tuesday-Thursday-Saturday. We’ll see how much this low dose every other day strategy lowers my LDL and ApoB. I may have to skip statins altogether. Bempedoic Acid and Ezetemibe work just fine with no side effects.
My wife doesn’t do very well with statins either. Her doc prescribed 40mg, she kept reducing because of side effects (weakness and forgetfulness), now she gets 5 mg and quarters them, 1.25mg per day (looks like a spec of dust). Despite the miniscule dose, it still keeps her ldl in check.
While I am sitting, my calf muscles begin to twitch uncontrollably for a few seconds and then stop. This can happen several times a day when I am taking a statin. It is also accompanied by soreness. However, my calves are the muscle that get the most exercise as I like to take the stairs and do soleus pushups. They’re currently the only muscles that spasm and only while on a statin. Both my parents suffer soreness and weakness from statins.
I have had similar spasms in other muscle groups many years ago when I wasn’t taking any supplements, medicines or statins.
Before giving up completely on statins, you could try one last hail mary, with pitavastatin 1-2mg. Supposedly, it has less impact on muscles. It is a good statin as far as effectiveness vs CVD outcomes, and if indeed it spares your muscles, that could be a win. It’s cheap and easily obtainable from India. I’d stick to Sun Pharma and Zydus.
I think I’ll try Atorvastatin 5 mg as I had bought a 2 year supply which is now 4 years on my Mon-Wed-Fri schedule. It’s not horrible. When I run out, I’ll try pitavastatin.
There’s also Fluvastatin, Pravastatin, Simvastatin, and Lovastatin. Maybe one of those you haven’t tried yet has the chemical composition just right for you to not to cause muscle pains when inhibiting HMGCR there.
Forgetfullness and just plain stupid on Rosuvastatin-really alarming -even on 2.5mg/day. Muscle pain so bad that I went to the ER and was told to stop. No forgetfulness on Atorvastatin but the muscles hurt like crazy. Tried Rapatha pcsk9i- developed severe cough/ Then tried 6month Inclisiran PCSK9i- sore muscles and joints-mood alterations and severe sensitivity to caffeine. Hope to try Bempedoic acid -but it’s not available in Canada. I take ezetimibe in between


{kind=link}