If LDL is low but triglycerides are high, with untreated diabetes, that probably means there were discordance between LDL and apoB and apoB was either normal or elevated. Having a normal or high apoB causes disease over time many decades, and diabetes is not good for anything and increases risk.
Any independent 3rd party validation of their claims? False positives?
"The Future”: the only marketed prognostic blood test for 1-year risk of heart attack (MI), stroke or cardiac death (MACE or major adverse cardiovascular events). Yielding an accuracy of 86%, HART CVE™ assesses four clinically significant blood proteins in a machine learning (AI) algorithm to calculate a patient- specific risk score. Proteins include:
NT-proBNP- associated with myocardial (heart) stress
Kidney Injury Molecule-1 (KIM-1)- associated with cardiorenal dysfunction and injury
Osteopontin (OPN)- associated with calcification and plaque formation
Tissue Inhibitor of Metalloproteinases-1 (TIMP-1)- associated with plaque rupture potential and left ventricular enlargement and dysfunction
The Here and Now”: diagnostic blood test for obstructive coronary artery disease. Yielding an accuracy of 86%, HART CADhs™ assesses three clinically significant blood proteins and three clinical variables (age, sex, history of coronary intervention) in a machine learning (AI) algorithm to calculate a patient- specific risk score of obstructive coronary artery disease. Proteins include:
hsTroponin- associated with myocardial ischemia and injury
Kidney Injury Molecule-1 (KIM-1)- associated with cardiorenal dysfunction and injury
Adiponectin- associated with glucose and fatty acid metabolism
Thomas Dayspring have said it’s a surrogate for apoB.
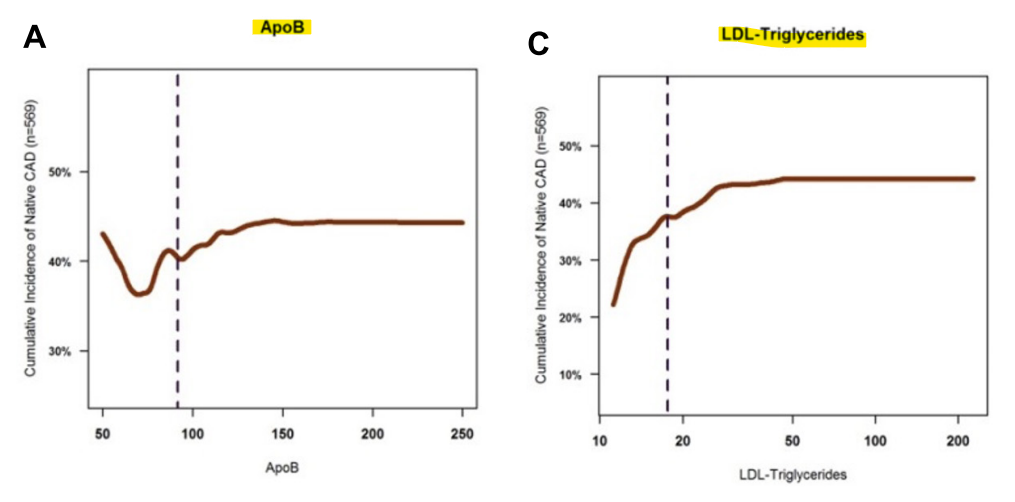
Thomas Dayspring might have said that, but the paper definitely does not. “Adjusting the model for age, sex, LDL-C and ApoB levels demonstrated that the association of LDL-TG with atherosclerosis was independent of these well-known factors [, including ApoB].”
Just look at the chart for the population in the study for ApoB and LDL-TG. You could be patting yourself on the back for having lowered your ApoB < 50 with statins, but your LDL-TG could still be elevated, increasing your CAD risk.
Looks like that study method is B.S. with a B.S graph.
50 apoB doesn’t have the same risk as 120 apoB. Just another fake U-shape curve with residual confounding.
It would be nice if there was a way to get LDL-TG from TG and LDL-C. I couldn’t find any resource online to do that. FWIW, I asked ChatGPT and got the following.
It is not possible to calculate LDL-TG (low-density lipoprotein triglycerides) directly from a standard lipid panel because such panels typically report:
Total cholesterol
High-density lipoprotein (HDL) cholesterol
Triglycerides
LDL cholesterol (calculated or measured)
The triglycerides reported in the standard lipid panel reflect all triglyceride-rich lipoproteins, not specifically those in LDL particles. LDL particles typically contain very little triglyceride, and LDL-TG levels are not routinely measured in standard clinical settings.
Methods to Estimate LDL-TG
To measure or estimate LDL-TG, specialized techniques like ultracentrifugation or nuclear magnetic resonance (NMR) spectroscopy are required. These methods separate LDL from other lipoproteins and allow for direct triglyceride content analysis.
If you’re interested in exploring this, it’s best to consult with a healthcare provider or a lipid specialist to discuss the need for advanced lipid testing.
EDIT: @adssx shares a way to estimate LDL-TG here.
But that’s only the estimated LDL-TG (eLDL-TG). If you want to find your real LDL-TG you need to test it but as you said it’s not commercially available in most labs.
They tend to stick less than small particles but contain more cholesterol so overall the net effect is the same for both types.
Imagine a cal 50 BMG round hitting you once or 9mm bullets hitting you 10 times. In both cases you’d end up dead.
It’s not the impact that matters most of the time, it’s the amount of bullets, so the 10 9mm bullets would be more harmful to the arterial wall in this context… that’s what apoB measures.
Not sure about LDL particle sizes. LDL-TG is a component of LDL, so maybe LDL size doesn’t matter as much?
Using your lipid values to estimate LDL-TG, I get 31 mg/dL. Per the paper, ideally you would want this below 20. In your case, the main target would be lowering triglycerides. But who knows, the estimate only has a R2 of 60%, so there’s a lot of room for error.
Statin update. It seems I am even intolerant to 5 mg of Atorvastatin. I switched to a Monday-Wednesday-Friday night dosing schedule and the muscle spasms stopped, but I still experience muscle weakness in my calves and thighs on Tuesday-Thursday-Saturday. We’ll see how much this low dose every other day strategy lowers my LDL and ApoB. I may have to skip statins altogether. Bempedoic Acid and Ezetemibe work just fine with no side effects.
My wife doesn’t do very well with statins either. Her doc prescribed 40mg, she kept reducing because of side effects (weakness and forgetfulness), now she gets 5 mg and quarters them, 1.25mg per day (looks like a spec of dust). Despite the miniscule dose, it still keeps her ldl in check.


{kind=link}