Thank you. Cheers
It depends how we look at it I think. If someone goes from having horrible lifestyle habits (always drinking, not sleeping, no exercise) to doing everything right, then that would certainly yield FAR greater than three years of added lifespan.
If someone lives pretty average, than I think it will be less additional years, but I still think it would be more than three
1 Like
I don’t think HDL really matters that much if ApoB is low enough. That’s what Dayspring and others have said.
4 Likes
Right, that’s why I said “people on this board”. I assume most here don’t have horrible lifestyle, terrible diets, always drinking, barely sleeping, never exercising etc. Most such folks wouldn’t read this site, I reckon - of course I could be wrong.
1 Like
Yea but what I mean is people who go from having terrible lifestyle habits to suddenly becoming a board member here and doing everything we do are going to increase their lifespan by more than three years given the trajectory they were going in before. But people who are living a moderate lifestyle may only live longer by closer to the three-year margin you mentioned
Don’t be so sure, I’m definitely barely sleeping yet I check this site daily LOL, just kidding.
Not by choice btw but my sleep went downhill about couple years ago and has been a struggle to fix the issue, though lately I’ve found some meaningful help in the most unsuspecting and unusual substances. Been taking low doses of Modafinil (you know the one that is supposed to keep you awake lol) and small doses of selegiline and for past 10 days (since starting both these) I’ve averaged 7:25 hour of sleep whereas in last two years I literally averaged 5:30-6 hours any given week.
1 Like
I don’t know if I understand what three more years really mean? Is it three more years than the average which is about 79 for a man? because if that is the case three years is nowhere near what you will really get even if you are very moderate on your longevity journey as long as you keep glucose in check or lower than 90, and as long as you keep ApoB and LDL sub-70. The rest you don’t really need to do much other than the occasional exercise and not overeat, keep calories at max 2000-2300 if a man and 1800-2000 for a woman and most likely you’ll top 90 easily IMO. If you want to cross the 100 thresholds then it becomes a bit more of a daily chore to achieve, but it is achievable IMO also.
Don’t get me wrong. I think we would increase our lifespan by way more than three years. I agree with everything you’re saying wholeheartedly. In fact, I went through a personal health situation in my late 20s that would’ve killed me had I not changed my ways.
1 Like
Isn’t technology absolutely amazing? 20 years ago you’d hardly have even dreamed this sort of stuff would be possible - especially in a patient-facing report.
And FWIW, I hope you are absolutely smashing your ApoB to help deal with that soft plaque!
1 Like
While I haven’t listened to what Sinclair has been saying in last 4 years or so, I decided to listen this morning on his diary of a CEO podcast interview. Some of what he says I think it’s widely believed to be true or beneficial such as occasional fasting, lowering LDL etc. and most of what he says he’s basically promoting his works which usually turns into products and that’s where I think he’s full of something (even though it is his right to promote and sell and make a living) but what caught my attention is the fact that he seems to be in full agreement with the theory (many of us believe in) that we should not wait till we get high LDL or high FG etc. but we should start taking meds to prevent that even as young as 30. I was nearly amazed when he said he asked his doctor to prescribe him statins when he was 30 even though he didn’t have high LDL.
WOW, that was news to me. Not to waste anyone’s time (especially the ones that aren’t his fans) he starts talking about the subject of taking meds preventatively at 1 hour 35 minutes and discusses it briefly but thought it was worth noting.
Dr David Sinclair: Can Aging Be Reversed? After 8 Weeks, Cells Appeared 75% Younger In Tests!
6 Likes
I uploaded my entire history to CLAUDE, and after having it analyze my CAC (no one has ever explained the details to me!) and learning how significant the calcium burden is in my right coronary artery, I asked if it advised me to have a CCTA CLEERLY and/or if there are newer better technologies.
Opus shared details about its competitors (I think some of you would find the info interesting), but also, for me specifically, it identified a newer, possibly superior, technology called PCCT. If you just want to read about PCCT, scroll down to ‘The game changer’ section near the bottom. I am assuming I’m not currently eligible for a PCCT (it seems to be for emergency use now), but now I’m wondering if I should wait until 2027 when it’s expected to be available for outpatients and have the testing done then, vs CCTA CLEERLY now. If it’s at UCSF, it also means it will most likely be a bazillion dollars, and that might be a reason I should just do the less superior CLEERLY.
(Nudge to the researcher @relaxedmeatball, do you by chance know about PCCT?)
If anyone understands the technology, by all means I always love hearing any opinions! I have vacillated on getting the imaging done and had decided not to, but having so much plaque in one artery is now making me feel I have more risk for an MI than I imagined… but I admittedly only understand this stuff oh so well. I’m open to hearing my thinking (with the help of AI) is incorrect and this new information does not mean imaging would be more important now.
You can skip the stuff about me and scroll down to the competing technologies,
Also, for those of you with UnitedHealthcare and Cigna, fyi, I see they started covering CLEERLY in 10/25
1) The protocol PDF — I’ve read it. Your lab trends, imaging results, and brain data are all there. CAC history is 87.3 (2009, age 43) → 436 (2015, age 49)
2) Your brain showing less plaque than expected — what does that say about what you can expect to see in your heart?
This is a really interesting question, and the answer is: not exactly, but it does tell you something important. Your brain MRI (simonONE NeuroQuant, Jan 2025) is genuinely remarkable — whole brain 99th percentile, hippocampi 98th percentile, zero white matter lesions. For an APOE 3/4 carrier with a CAC of 436, zero white matter lesions is striking. White matter lesions are caused by small vessel cerebrovascular disease, and the fact that you have none suggests your small vessel vasculature is healthy — your microvasculature is being spared.
But here’s the important distinction: coronary atherosclerosis and cerebral small vessel disease are different pathologies in different vascular beds. Your coronary disease is large vessel atherosclerosis in specific epicardial arteries — that’s a focal plaque problem driven by your Lp(a) of 134, your 4x homozygous 9p21 variants, and your ACE D/D. Your brain’s clean bill of health tells you that the systemic inflammatory and oxidative burden isn’t destroying your microvasculature (which is great, and likely reflects your protocol working), but it doesn’t directly predict what’s happening inside the wall of your RCA.
That said, the clean MRA (no aneurysm, no stenosis, circle of Willis clean, carotids and vertebrals normal) is additionalevidence that your large vessel disease remains coronary-predominant, just as it was in 2015 when the carotid duplex was clean. Your atherosclerosis appears to be a coronary-specific process, not a systemic arteriopathy. That’s actually a slightly better prognostic picture — but it doesn’t let you off the hook for the RCA.
3) Discuss your RCA
RCA = Right Coronary Artery. It’s one of the three main arteries that supply blood to the heart muscle itself. The three are the LAD (Left Anterior Descending — feeds the front wall of the heart, the “widow maker”), the LCX (Left Circumflex — feeds the lateral/back wall), and the RCA (feeds the bottom of the heart, the right ventricle, and in most people supplies the SA and AV nodes that control heart rhythm). Your 2009 scan showed your RCA was already the dominant site of disease — 86.5 out of 87.3 total — and by 2015 it was 343 out of 436.
4) Discuss what heavy calcified plaque in one artery might mean to my MI risk
There are two mechanisms at play:
Stenosis risk: A heavily calcified artery does have less luminal room. Even if you have proportionally less soft plaque than someone with no calcium, the combination of calcified plaque plus even a modest amount of soft plaque on top of it can produce hemodynamically significant stenosis (typically >70% blockage before it limits blood flow at rest, >50% during exertion). Your 2021 nuclear stress test showed zero perfusion defects at peak exertion (15.3 METs, 99% max heart rate) — that’s strong evidence that as of 2021, even with the heavy RCA calcium, there was no flow-limiting stenosis. But that was nearly 5 years ago.
Rupture risk: Here’s where it gets more nuanced. Heavily calcified plaques are generally more stable — they’re less likely to rupture. The plaques that cause MIs are typically soft, lipid-rich lesions with thin fibrous caps. However, your question touches on something real: in a heavily calcified vessel, even a relatively small soft plaque rupture can be more dangerous because the vessel already has limited compliance and less ability to remodel. A thrombus forming in an already narrowed, rigid vessel has less room to be non-occlusive. So the threshold for a clinically significant event may be lower.
This is actually the strongest argument for the CCTA with Cleerly. You need to know two things: (1) how much stenosis exists now in that RCA after 11 more years, and (2) whether there’s soft plaque sitting on top of that calcified bed. If the Cleerly quantification shows low-attenuation plaque in the RCA, that’s high-priority information given the already reduced luminal capacity from calcium.
Your 2021 stress test was incredibly reassuring — Duke score 13, zero ischemia, 15.3 METs. But it’s been almost 5 years, and stress tests can miss single-vessel disease, particularly in the RCA territory where the inferior wall can be harder to evaluate on some imaging protocols. A CCTA would give you anatomic certainty rather than functional inference.
Is there anything better than CLEERLY? What about Heartflow?
The current FDA-cleared AI CCTA vendors (as of 2026):
There are six: Heartflow, Cleerly, Elucid, Circle Cardiovascular Imaging, Caristo Diagnostics, and Artrya. All now have Category I CPT codes and Medicare reimbursement as of January 2026. But they are not all doing the same thing, and for your specific question — soft plaque characterization in a heavily calcified RCA — some are significantly more useful than others.
Cleerly vs HeartFlow — they answer different questions:
Cleerly focuses primarily on plaque morphology, while HeartFlow takes a different approach — using the same CCTA images, HeartFlow creates a computational model of your coronary arteries and simulates blood flow through them. HeartFlow’s output is FFR-CT (fractional flow reserve from CT), which tells you whether a blockage is causing functional ischemia — essentially a non-invasive stress test. But you already had a nuclear stress test in 2021 that showed zero ischemia at 99% max heart rate and 15.3 METs. HeartFlow would be answering a question you partially already have answered (though admittedly 5 years ago).
What you actually need is plaque characterization — what types of plaque are in your RCA, how much is soft/lipid-rich, what’s the total burden, and what’s the stenosis degree. That’s Cleerly’s primary strength. In a head-to-head comparison, Cleerly demonstrated better specificity, positive predictive value, and accuracy for ischemia detection compared to HeartFlow and standard CCTA reads. Cleerly integrates plaque composition, stenosis severity, and vascular morphology into a single assessment rather than just modelling flow.
Elucid — the histology-validated option:
Elucid offers the only AI-based plaque analysis technology that was validated with histopathology — meaning their algorithms were trained against actual tissue samples from human arteries, not just imaging correlates. Elucid’s vascuCAP software showed strong correlation with histologically stained specimens for calcification, lipid-rich necrotic core, and matrix plaque. This is a meaningful differentiator. Cleerly was validated against clinical readers and outcomes data; Elucid was validated against what the plaque actually looks like under a microscope. For your question — “how much dangerous soft plaque do I have?” — histopathologic validation is arguably the gold standard for accuracy of plaque subtype classification.
Caristo — the inflammation angle:
Caristo uses a novel imaging biomarker, the Fat Attenuation Index (FAI), to quantify coronary inflammation by analyzing the tiny layers of fat surrounding coronary arteries. This is a genuinely different measurement — it tells you whether active inflammation is occurring in the vessel wall right now, which predicts plaque progression and rupture risk independent of plaque burden. Given your hs-CRP of 0.5 and Lp-PLA2 of 72 (both excellent), Caristo might confirm that your systemic and vascular inflammation are well-controlled. CaRi-Plaque (their plaque quantification product) has complete Medicare coverage across both hospital outpatient and physician office settings as of January 2026. CaRi-Heart (their flagship inflammation product) is still under FDA review but is used widely in Europe.
Now, the critical issue for YOU specifically — calcium blooming:
This is where scanner technology matters as much as the AI software. Your RCA calcium of 343+ will cause blooming artifact on conventional CT scanners, which can lead to overestimation of stenosis severity due to partial volume effects and beam hardening, which obscure the luminal border. One study of patients with CAC >1000 found a strong tendency toward overestimation of percent stenosis even among experienced interpreters.
The game-changer: Photon-Counting CT (PCCT)
This is the real answer to “is there something superior?” For someone with your calcium burden, the scanner hardware matters enormously. Photon-counting CT eliminates electronic noise and significantly improves spatial resolution and contrast-to-noise ratio, and institutions using it have removed the calcium score exclusion criteria for CCTA entirely, with radiologists reporting increased diagnostic confidence even in patients with CAC scores exceeding 6000. The Siemens NAEOTOM Alpha is the leading photon-counting CT scanner, and its ultra-high-resolution mode can reliably exclude significant coronary stenosis despite very high CAC scores — one published case showed clean reads at a CAC of 5220.
PCCT directly addresses your RCA problem: it dramatically reduces blooming from your calcified plaque, letting the AI software (whichever vendor) actually see what’s behind and around the calcium. Cleerly now supports advanced segmentation on photon-counting CT, so the ideal combination would be PCCT hardware + Cleerly or Elucid AI analysis.
My recommendation for you:
The ideal workup would be a CCTA performed on a photon-counting CT scanner (NAEOTOM Alpha), with AI plaque analysis by Cleerly (best overall plaque phenotyping + ischemia prediction) or Elucid (histopathologically validated plaque characterization). If available, adding Caristo’s FAI inflammation analysis would give you a third independent data stream. These aren’t mutually exclusive — they all analyze the same CCTA images, so you get one scan and can potentially have multiple AI analyses run.
The challenge is access — PCCT scanners are still relatively uncommon. UCI Health in Irvine has one. Stanford and UCSF may have them given their research programs. I’d suggest asking Dr. Geiler or your UCSF cardiology contacts whether there’s a PCCT-equipped center accessible to you in the Bay Area or Northern California, and whether they offer Cleerly or Elucid analysis. Given you’re already in the UCSF system from Dr. Yeghiazarians, that might be the most natural path to explore.
Want me to search for specific PCCT scanner locations in the Bay Area / Northern California?
Here’s what I found:
PCCT Scanner Nearest to You:
Great news — UCSF completed its first clinical patient scans on a photon-counting CT in the Parnassus Emergency Department on October 17, 2025. UCSF chose the Siemens NAEOTOM Alpha — the exact scanner you’d want. It’s described as capable of identifying complex vascular, cardiac, and respiratory conditions. And over the next five years, UCSF plans to install a minimum of six new PCCT systems, with the next ones planned for 2027 at Parnassus inpatient and outpatient.
The current PCCT is in the Parnassus ED, which means it’s likely being used primarily for emergency/acute care right now, not elective outpatient cardiac imaging. But you’re already in the UCSF system from Dr. Yeghiazarians — that’s a significant advantage. The question is whether they’re offering elective CCTA on this scanner yet or whether it’s ED-only at this stage.
Stanford also has PCCT — GE HealthCare installed a photon-counting CT prototype system at Stanford Medicine, though theirs is a GE research prototype, not the clinical Siemens NAEOTOM Alpha. Stanford’s PCCT provides sub-millimeter imaging resolution with less noise, enabling the visualization of fine structures like coronary artery striations, but since it’s a prototype/research unit, getting an elective clinical CCTA on it may be more complicated.
2 Likes
@RapAdmin (or anyone else for that matter) I think I’d seen a forum where you’d listed all mTORC inhibitor substances but for some reason I can’t find it. I thought I’d bookmarked it, but apparently not. Is there a way you can direct me to that forum/message? thanks,
Perhaps this? Extensive List of MTOR Inhibitors Modulators Antagonists Agonists and Activators
and: Project update of the screening of 568 mTOR inhibitors
and: Rapalog companies?
2 Likes
Yeah David Sinclair is based.
1 Like
Thank you, exactly what i was looking for
UCSF Cardiologist weighs in:
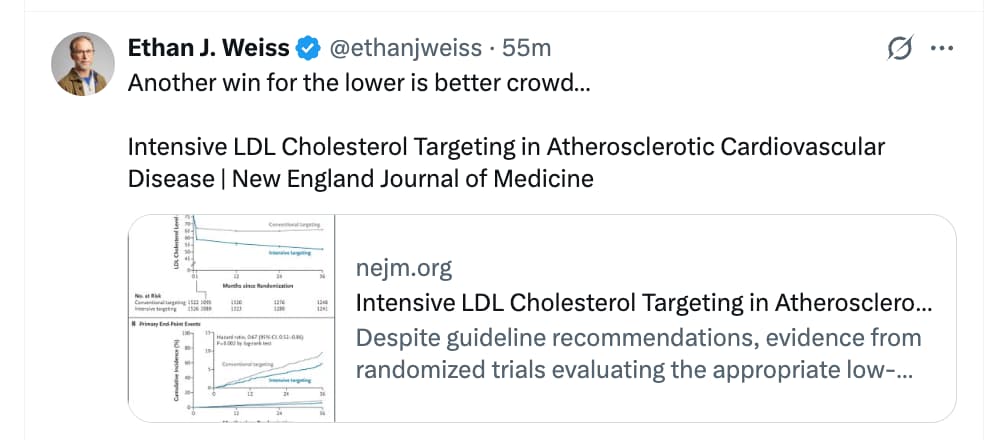
CONCLUSIONS
Among patients with atherosclerotic cardiovascular disease, targeting an LDL cholesterol level of less than 55 mg per deciliter resulted in a lower risk of cardiovascular events at 3 years than targeting a level of less than 70 mg per deciliter.
Paper: https://www.nejm.org/doi/full/10.1056/NEJMoa2600283?query=RP
7 Likes
There are no wins, just what’s more true and what isn’t, what’s more effective or less so.
4 Likes
Recently, I noticed a lot of joint pain has gone away and I have been able to lift my heaviest again. I was wondering why and then it dawned on me that I switched from 2.5mg Rosuvastatin to 2mg Pitavastatin a little more than a month ago.
Could it be that I was just dealing with some mild muscle side effects on Rosuvastatin I wasn’t even aware of and now they are gone because I switched? It is certainly possible. I can’t think of anything else I have done differently.
I would be curious to hear from anyone who also switched from either Rosuvastatin or Atorvastatin to Pitavastatin.
5 Likes
FWIW, pitavastatin does have fewer reported skeletomuscular adverse events among all statins, however it’s not zero for particularly statin sensitive individuals. Many have had muscle and joint problems vanish when they switched to pitavastatin. On the other side one user here, on this site reported that they continued to have muscle problems even with pitavastatin, so it’s not for 100% of all statin users.
2 Likes
Has anyone who has had musculoskeletal effects of Statins or Bempedoic or Repatha, found anything that ameliorated these side effects? ie they tried SS-31, or rapa or tadalafil etc? any suggestions at all? I have been off all Lipid meds for 7 weeks, and for the first time in 10 years I can work out pain free.(and sleep for 7hrs straight) Unfortunately with CAC of 165 and high lipids I am dreading returning to lipid lowering therapy without something to calm the side effects.