I can’t speak to your particular doc, but I’ve never had a doctor deny me anything I’ve asked for (I have good docs, I’m very assertive, and don’t ask for anything that is not appropriate for me, so my experience could of course be different)
My insurance sorta kinda covers it, but I have an 8k deductible, so I’m paying mostly out of pocket, unfortunately.
I do get a coupon from them, so for a few months per year I only pay aprox $15.
I’d see if you are eligible for the coupon and consider what some others have done… just use it on occasion to make it last?
Or perhaps your insurance is better, so it’s worth looking into .
I meant from purchasing from a generic manufacturer or India if they were available there.
I wasn’t aware of this graph. How reliable is it, and what about in the most recent years? Just curious.
Manufacturing costs might also differ depending on the mAb.
Objective: To resolve the historical inconsistency regarding the cardiovascular benefits of Omega-3 fatty acids (EPA and DHA) by conducting a meta-analysis that specifically evaluates the relationship between dosage and cardiovascular outcomes.
Methods: The authors performed a systematic review and meta-regression of **40 randomized controlled trials (RCTs)**involving a combined total of 135,267 participants. They analyzed the effects of EPA and DHA supplementation on myocardial infarction (MI), coronary heart disease (CHD) events, CVD events, and mortality.
Key Findings:
supplementation was associated with a statistically significant reduced risk of:
Dose-Response: The study identified a linear dose-response relationship. An additional 1000 mg/day of EPA/DHA was associated with an additional 9% reduction in the risk of myocardial infarction (P < .001) and a 5.8% reduction in total CVD events (P < .001).
Conclusion: Omega-3 supplementation is an effective preventive strategy for CVD, with benefits that increase with dosage. Previous conflicting studies likely failed to show benefit due to insufficient dosing.
Midlife Mediterranean diet is associated with subclinical carotid atherosclerosis in late midlife
Conclusion
Findings underscore associations of midlife Mediterranean-style diet and lower presence of subclinical carotid atherosclerosis at Age 60 and confirm the significance of dietary interventions as potential means for cardiovascular disease prevention. The study enhances understanding of long-term dietary patterns and their link to subclinical atherosclerosis, supporting future interventions and further research.
MDS & Plaque: High or midrange cumulative MDS across midlife was significantly associated with a reduced prevalence of carotid plaque at age 60 (OR ~0.72–0.74) compared to low adherence.
Sex-Specific Divergence:
Women: The association between higher MDS and reduced plaque was strongly driven by women (OR: 0.41).
Men: A significant association between MDS and CIMT (wall thickness) was observed only in men.
Null Result for HDS: The generic “Healthy Diet Score” showed no significant association with either plaque or CIMT, suggesting that specific components of the Mediterranean diet (e.g., lipid profile modulation, anti-inflammatory properties) are superior to general “healthy eating” guidelines for this specific vascular outcome.
I believe so. Whenever I’ve taken it, I have noticed zero side effects (besides dark stools) and it reliably increased my ferritin quickly. It can be taken with or without food and still be well absorbed.
Atherosclerotic cardiovascular disease (ASCVD) is the leading cause of morbidity and mortality worldwide, and LDL-cholesterol (LDL-C) plays a fundamental causal role. The classic INTERHEART study showed that dyslipidemia, characterized by an elevated apolipoprotein B/apolipoprotein AI ratio, was the risk factor with the highest population-attributable risk (PAR) for myocardial infarction (MI) (PAR 49.2% for the top four quintiles vs. the lowest quintile).
Despite strong evidence supporting the benefits of statins in reducing ASCVD, misinformation about this therapy continues to spread widely on social media, potentially increasing the risk of clinical events for the population. A Danish study showed that early statin discontinuation was more common after exposure to negative media coverage and was linked to a higher risk of MI and ASCVD death. Misinformation is a threat that needs to be fought because it causes delays in starting lipid-lowering treatment, denying many patients its benefits.
AI and Genetics Reveal Early Risk Signals for Aortic Stenosis
Aortic stenosis is one of the most common and deadly forms of heart valve disease, affecting millions worldwide. The condition develops gradually as the aortic valve narrows, eventually limiting blood flow from the heart. Yet despite its prevalence, medicine still lacks drugs that can prevent or slow its progression. Once the disease becomes severe, patients are left with only one option: valve replacement through surgery or catheter-based procedures.
A new study from researchers at UC San Francisco and the Broad Institute of MIT and Harvard suggests that this reactive approach may not be inevitable. By combining artificial intelligence–based imaging analysis with large-scale human genetics, the team has uncovered early genetic signals that shape aortic valve function long before clinical disease develops. The findings, published in Nature Genetics, point toward a future in which aortic stenosis could be detected, and potentially intercepted, years earlier.
Greetings, I am afraid I cannot give you a ‘protocol’ that I followed. The gap between testing was about 15 years. Only one factor remained constant. I do a blood test every six months or so and I have maintained the LDL levels almost always below 50 and Apo B below ~60. Lately it (LDL) has been below 30 (below 20 also for a year). I attribute this to effect of polypharmacy (Quercetin, Fisetin…). No irrefutable proof.
No butter, vegetarian diet, Diabetic (gross and yet!). Little formal exercise, keep moving (not at all sedentary) Last two years was on Nattokinase, Serrapeptase and Lumbrokinase and whatever else I read about. Nothing rigorous or scientific about anything, I stick to a supplement for at least 6 months. Brownian motion with a directional bias! More focused on my diabetes the last few years. I take notes but I misplace them/lose them. Life goes on and another New Year dawns!
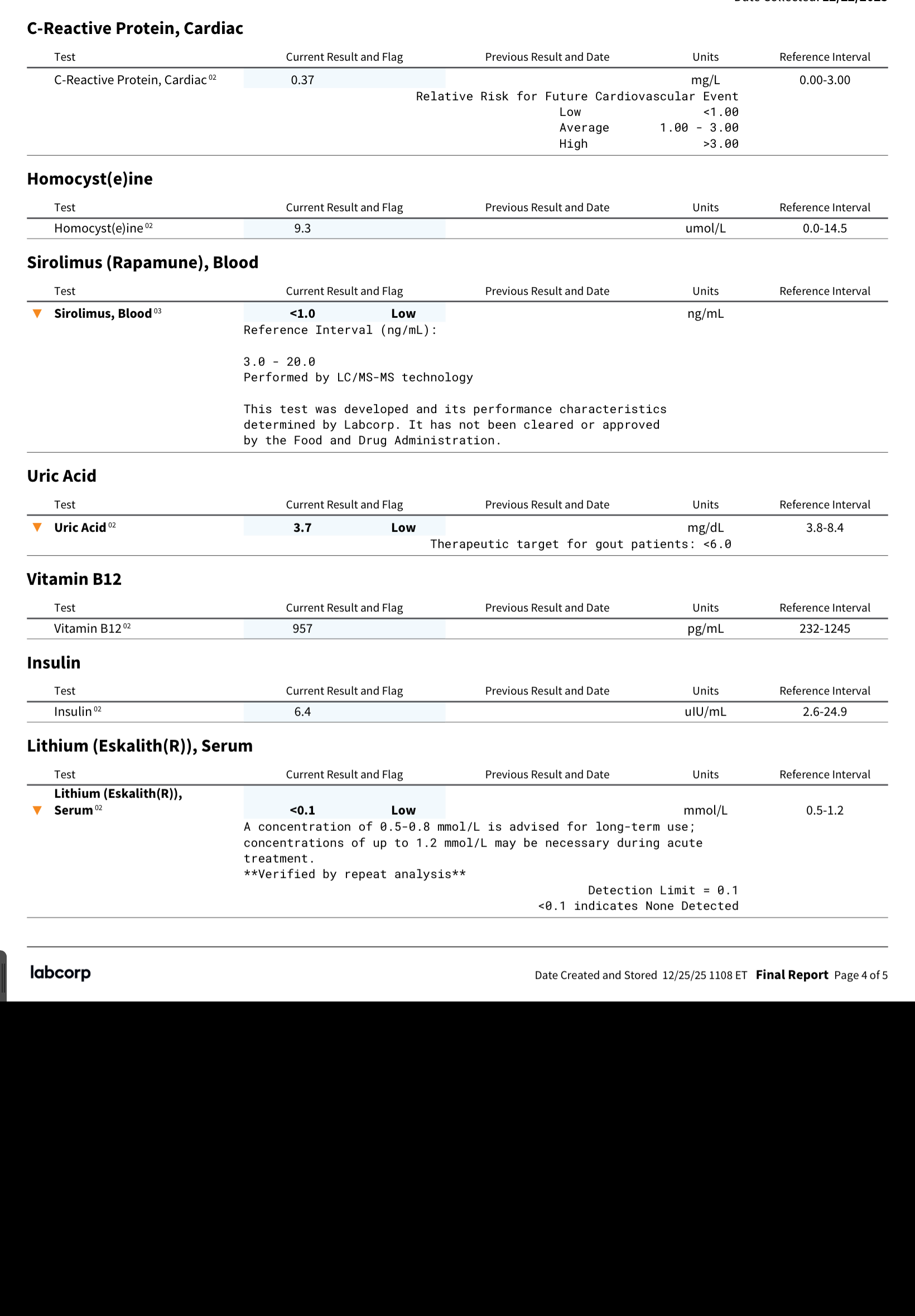
I got some blood tests from LabCorp just before my ACDF surgery, to make sure my sirolimus levels were zero. While at it I also took the opportunity to get some other tests, including ApoB, which I didn’t get back in October at UCLA. So, this is while on 4mg pitavastatin, bempedoic acid 180mg + ezetimibe 10mg. However, at the point of the test I was no longer taking empagliflozin, telmisartan or rapamycin (in preparation for the surgery).
My results:
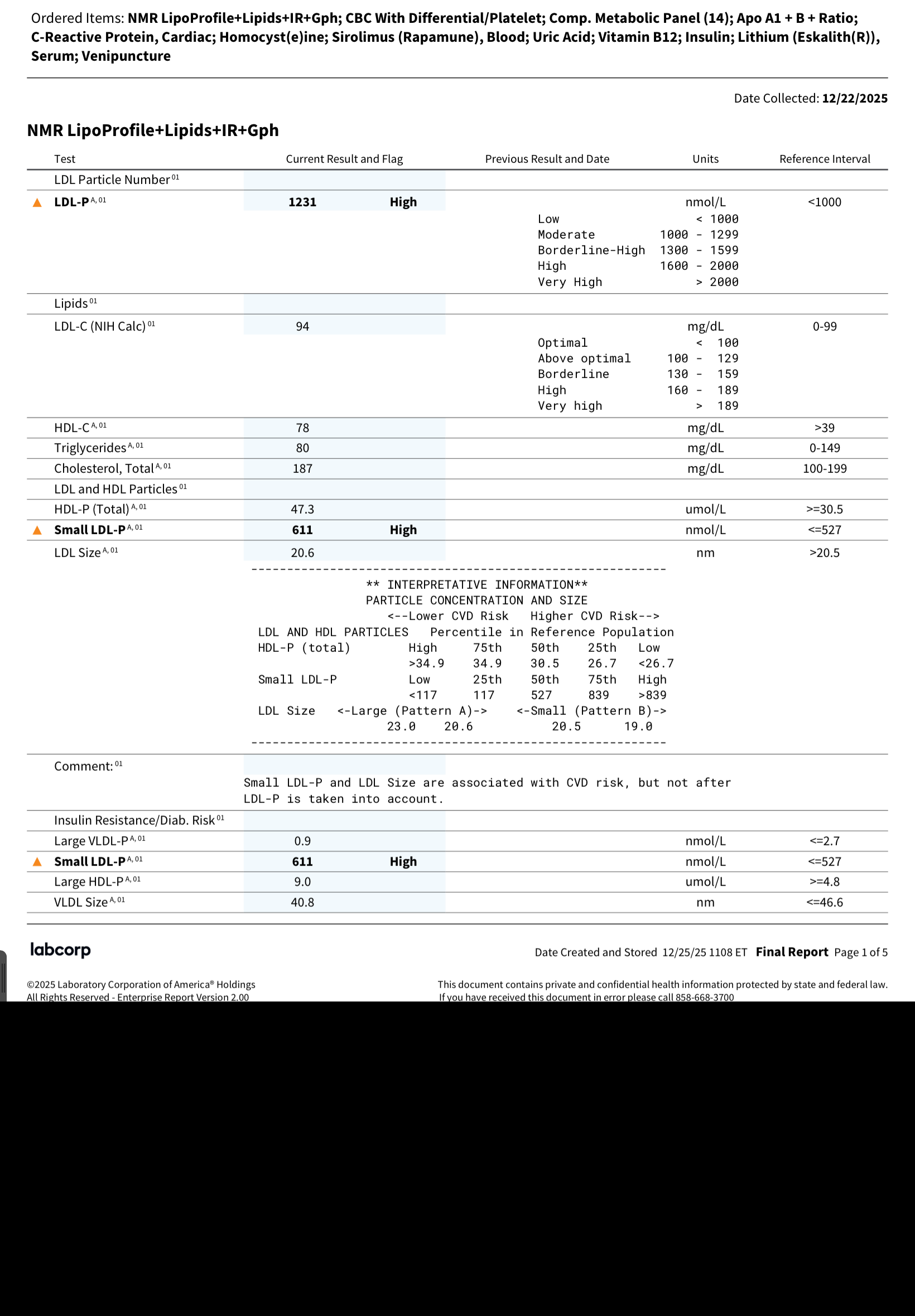
TC - 187 mg/dL
LDL-C - 94
HDL-C - 78
TRG - 80
So, pretty garbage.
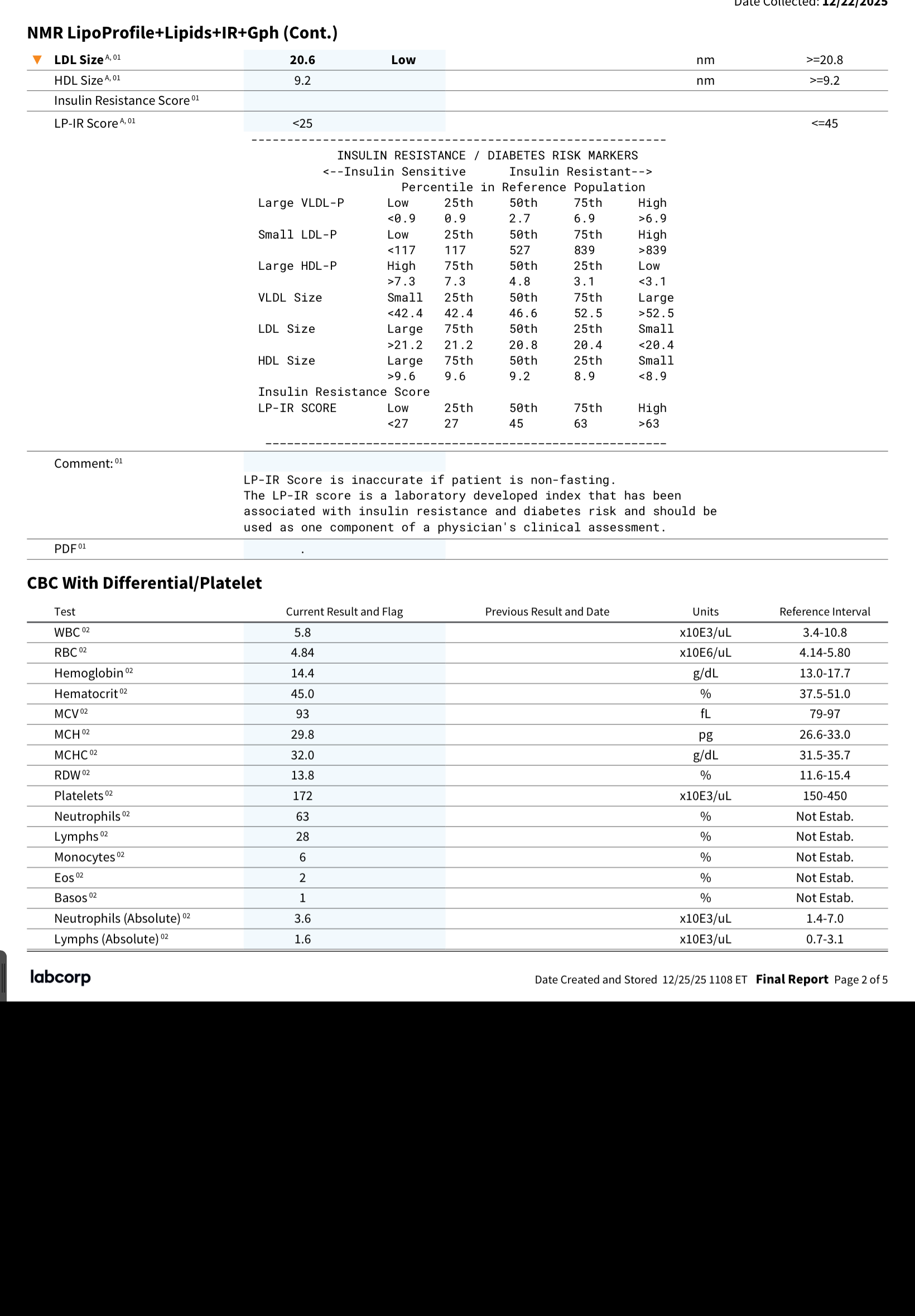
ApoB - 76
ApoA-1 - 192
Barely acceptable.
Other lipid numbers: continue to be absolute trash.
LDL-P (particle number) - 1231 nmol/L
Small LDL-P - 611
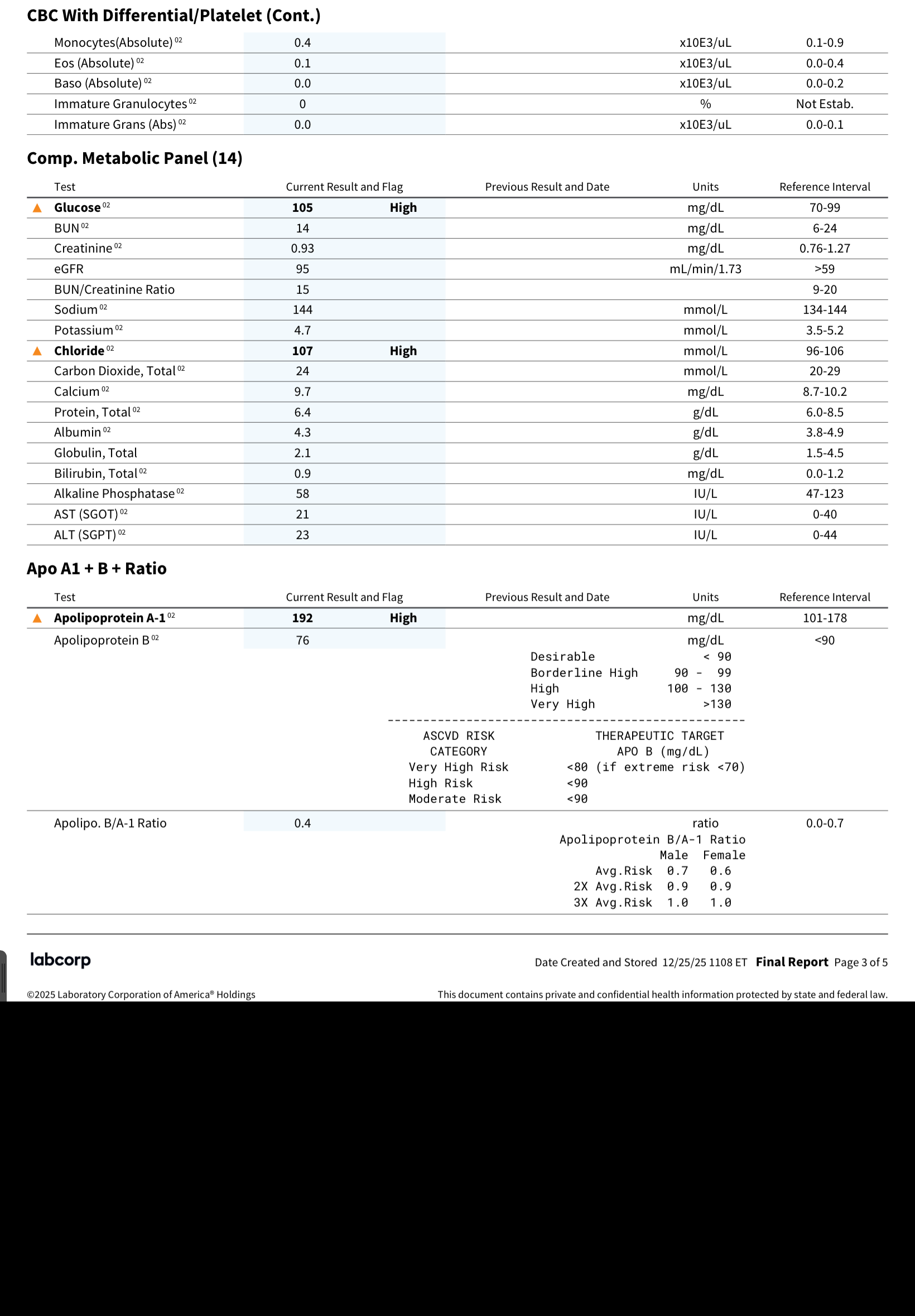
LDL Size - 20.6 nm
Can’t say I understand much of these numbers. How can my ApoB be at 76, when not only is LDL-C at 94, but my trigs are at a hefty 80, and the LDL-P is high, as well as small LDL particles are high and overall LDL size is “small”. AND my Lp(a) is always insanely sky high. I don’t get it. Taken together I’d imagine my ApoB must be much higher than 76. I’m starting to think LabCorp is not reliable.
My fasting insulin is at 6.4 uUI/mL with fasting glucose 105 mg/dL; hscrp jumped up to 0.37.
All in all, I’m not pleased with my lipid numbers on triple LLT: pita + BA + EZ. I’m thinking about PCSK9i, but really waiting on new drugs. Cr@p.
I find it very surprising that your LDL-C is that high considering you’re taking all three meds that are supposed to crush it. As far as Apo-B it doesn’t seem to always be related to lipids. I have same scenario, my lipids are a bit high (naturally without any meds), but Apo-B is normal and that is a good thing since the Apo-B seems to be the new LDL-C meaning most doctors see high Apo-B as a better indicator of a potential future CVD event.
p.s why Labcorp if goodlabs is at least 30% cheaper, unless your tests are covered by you insurance.
ApoB is literally the lipid transport protein count. LDL can be confounded by size vs particle count. ApoB is supposed to get around that by collecting all the transport proteins into one number. Which is why I can make no sense of my numbers as I outlined above. It’s not simply the common discordance with LDL, but the particle count of all those proteins (including IDL). Re: labcorp, I was in a hurry and used Marek (who use labcorp) out of inertia as I already had an account with them. For my next test I do intend to look into Goodlabs.
Ah I see. Marek might have a special deal with Labcorp so you might have still gotten good prices, but it is not available in NY (where I live). In NY the cheapest by at 30% is goodlabs.