No, I started the Nexlizet after doing the first experiment w/LR3 and Nexlizet should have negligible effect on Lp(a) anyway.
I do want to emphasize that I do NOT recommend people run out and start injecting IGF-1 LR3. It hasn’t even passed phase 1 clinical trials, much less phase 2 or 3, and that’s assuming the LR3 you buy is pure and uncontaminated. We have safe and even more effective Lp(a) drugs coming out within the next couple of years. This was just some self-experimentation proof-of-concept work, and I have a higher than normal risk tolerance for this kind of thing.
I was trying to ask the opposite, meaning…if lr3 could lower your lp(a), could it have lowered your LDL . I assume you’ve already ruled that out.
Thx for the warning, and I wouldn’t run out and try this because I’m cautious about doing anything to increase the risk of cancer, and I’d want to understand it more.
Having said that, if this could potentially work with a very short term therapy and be lasting, then it’s something I might talk to my doc about….not that he would approve of me taking a research peptide, but he knows I do and he’ll at least go over things with me. But if this becomes worth considering, I wonder it’s it’s after a whole body MRI and a Galleri blood test.
Oh good question, that is indeed a possibility. I’ve stopped the LR3 and will be monitoring Lp(a) and my other lipids every 2 weeks to see how long it takes it to come back to my “normal” (i.e. high), so we’ll see if LDL/ApoB trends up as well.
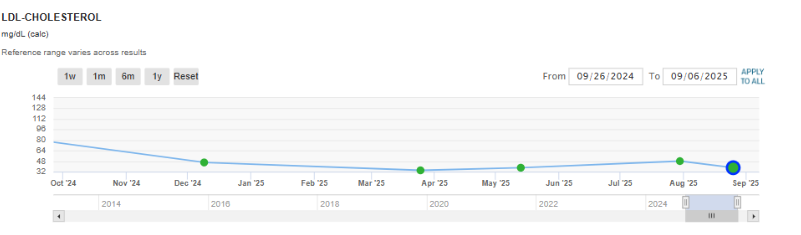
Brillo-EZ from Sun Pharma certainly worked for me. I was on atorvastatin 40 mg tablets for years, and it kept my LDL in the 70-80 mg/dL range. My doctor thought that was just fine and would not raise the dose or prescribe any adjunct meds like Brillo. I bought Brillo-EZ from Jagdish and paired it with atorvastatin, and it lowered my LDL cholesterol to below 40 mg/dL.
Stratifying cost benefit by purchasing power is an interesting and under-discussed aspect of precision medicine. I sometimes wonder if all the DTC lab test verticals and DTC specialist verticals are not just using direct pay to side-step insurance but also innovating on the margin of preventing moral injury to caring doctors who don’t want to give different advice to patients based on ability to pay. If there is a gating function that charges up front, you can order tests and write scripts without hesitation. If you are treating e.g. a mostly Medicare population, you’re probably going by population guidelines.
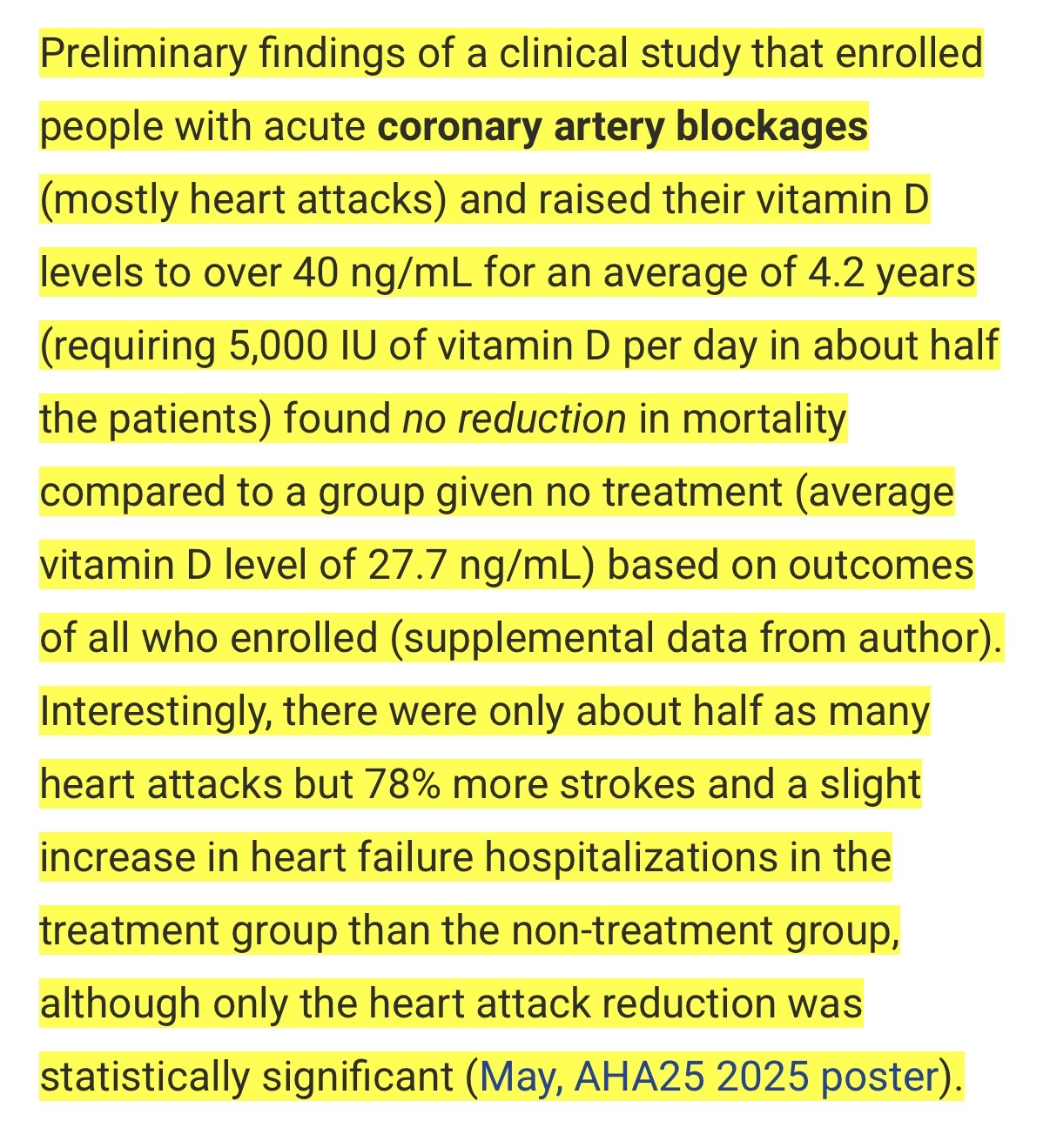
Consumerlab just added context to the study for those of us like me who didn’t take the time to really dig into it. This makes the results slightly less impressive.
Yes, but the study was with already sick people, not a healthy group that had been taking large amounts of vitamin D for years before any heart-related issues.
If the Lp(a) does return back to the high level after stopping LR3, you should consider trying to publicise this. Maybe a case report?
The study wasn’t powered for mortality. Most MIs are not fatal, so you will detect a change in MI frequency much easier than you’d detect a change in mortality. To get the change in mortality, you need a lot more than 600 patients, or you’d need an insanely high base mortality rate and a huge effect of Vitamin D, which seems unlikely.
And even so - an MI is still a life-changing event for people. There’s the obvious cardiac damage which will never recover, but it also greatly increases your risk of heart failure, or of having another MI in the future. You want to avoid the first MI as strongly as possible IMO.
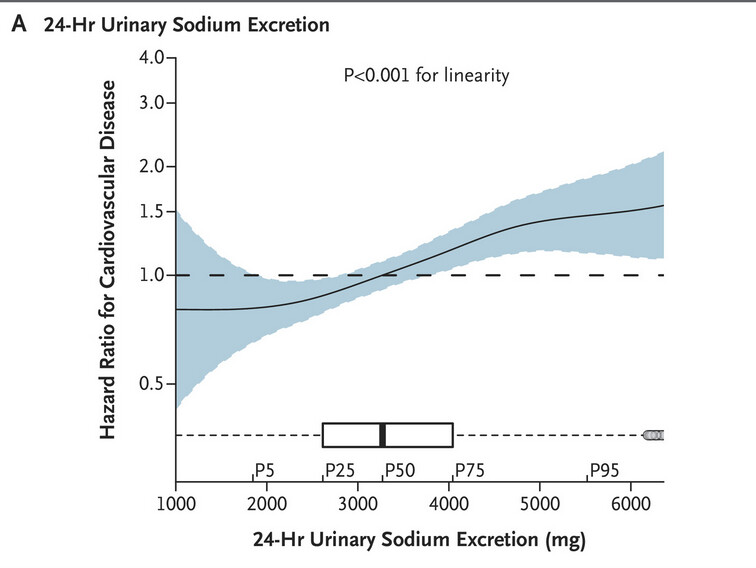
Higher sodium excretion, lower potassium excretion, and a higher sodium-to-potassium ratio were all associated with a higher cardiovascular risk in analyses that were controlled for confounding factors (P≤0.005 for all comparisons). In analyses that compared quartile 4 of the urinary biomarker (highest) with quartile 1 (lowest), the hazard ratios were 1.60 (95% confidence interval [CI], 1.19 to 2.14) for sodium excretion, 0.69 (95% CI, 0.51 to 0.91) for potassium excretion, and 1.62 (95% CI, 1.25 to 2.10) for the sodium-to-potassium ratio. Each daily increment of 1000 mg in sodium excretion was associated with an 18% increase in cardiovascular risk (hazard ratio, 1.18; 95% CI, 1.08 to 1.29), and each daily increment of 1000 mg in potassium excretion was associated with an 18% decrease in risk (hazard ratio, 0.82; 95% CI, 0.72 to 0.94).
The ratio of a person’s waist measurement compared to their height is more reliable than body mass index (BMI) at predicting heart disease risk, according to new research from UPMC and University of Pittsburgh physician-scientists.
This finding, published Oct. 31, 2025, in The Lancet Regional Health—Americas, could reshape how clinicians and the public assess cardiovascular risk, especially for people who don’t meet the classic definition of obesity.
The team analyzed data from 2,721 adults who had participated in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). The individuals had no cardiovascular disease at baseline and were followed for more than five years.
“Higher BMI, waist circumference and waist-to-height ratio at baseline were all associated with higher risk of developing future cardiovascular disease—until we adjusted for other classic risk factors, such as age, sex, smoking, exercise, diabetes, hypertension and cholesterol,” said lead author Thiago Bosco Mendes, clinical instructor of medicine at Pitt and obesity medicine fellow at UPMC. “When we did that, only waist-to-height ratio held as a predictor.”
Much of that predictive power is concentrated among individuals with a BMI under 30, which is below the classic threshold for obesity, who may not realize they are at risk for cardiovascular disease.
BMI doesn’t account for fat distribution or distinguish between harmful, visceral fat and protective, subcutaneous fat. By contrast, waist-to-height ratio (WHtR), calculated by dividing waist circumference by height, directly reflects central obesity, which is more closely linked to heart disease. That means that people with a BMI lower than 30, but a WHtR over 0.5, may be at higher risk of future coronary artery calcification, a key marker of cardiovascular disease, even in the absence of other risk factors.
What you’d want to do is collaborate with a researcher who can get permission from their university ethics committee to include your test results etc. Case studies are often reported about people doing “off-label” things.
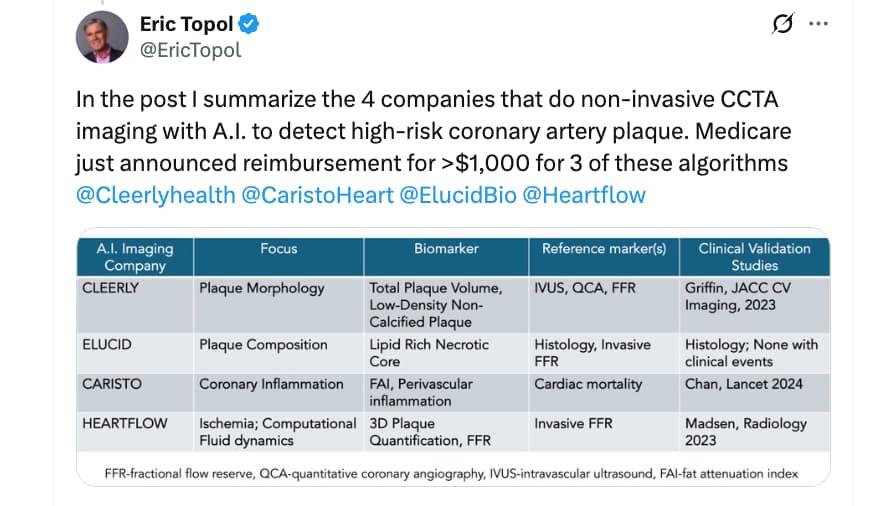
This year we’ve gotten signals that a major shift is ongoing, from fixation on obstructive coronary artery disease (simply put “blockages”) to the focus on non-obstructive arterial disease (simply put “atheroma”), as visualized non-invasively to be high-risk, so-called vulnerable atherosclerotic plaque, and/or exhibiting inflammation (Figure below). This Ground Truths edition will take you through the evolution of the thinking and capabilities, with new non-invasive A.I. imaging, and new drugs, that may ultimately lead to a major reduction in heart attacks.
Although statins have helped reduce the risk of heart attack, we still have over 800,000 each year in the United States, which is similar to the data spanning 2012 to 2022, and heart disease remains the number 1 killer despite a marked reduction in death rates over the past 2 decades. Even with 1 in 4 Americans taking statins now, it’s clear we’re far away from their disappearance. One prescient note in the Science editorial was “The challenge is to develop noninvasive screening methods to detect coronary atherosclerosis in its earliest stages.”
I take donotage’s sirt 6 activator and sirt 6 is said to lower ldl too… and this month I’m looking at getting on retatrutide finally - and that is said to too