The CTCA involves more cost - regionally $311-$600 cash pay through MDSave.com, but with a physician order.
CT Cardiac Calcium is $45-$200 typically.
There is more radiation exposure, need for an IV and exposure to contrast with the CTCA.
So I take a look at people who are very low risk of having any disease - and a CT Cardiac Calcium is sensible. Any non-Zero score gets a CTCA.
I have a lot of patients who have had CTCA’s including those with high calcium scores - and the results are useful and interpretable. In areas of heavy calcification in the vessel wall, we still usually see the vessel nicely, but it can limit interpretation. Adding Cleerly is of value in these cases or in cases where there is a reasonable plaque burden.
I don’t think that’s the best criticism of the study, it’s a observational study like many others and they controlled for a few factors (and Lp(a) and hsCRP). You can see the CI’s widening below the 5th percentile. If the methodology allowed for it then the short term would suggest no effect long term because it was statistically significant according to the authors.
Our analysis (Figure) also suggests that the relationship of LDL-C to MACE tends to flatten below ≈90 mg/dL, the range encompassing most patients in the triglyceride-lowering trials, although the wide CIs at the lower range of LDL-C do not exclude a monotonic relationship across the full LDL-C range.
A flattening of LDL-C with MACE or increase in all-cause mortality happens all the time in studies with this design, contrary to RCT’s.
What’s the added value of the CTCA in terms of treatment? With a positive calcium score isn’t the ideal treatment aggressive lipid lowering through medication and diet and exercise? So how would CTCA results change that? E.g. my understanding is that studies show that preventative angioplasty is virtually never warranted.
The value add is #1 Many times a CT Cardiac Calcium Score is elevated and yet there is no coronary artery disease in the lumen of the arteries. For example, in 2021 I had a CT Cardiac Calcium of 92 all focused proximal LAD. Late 2021 I got pericarditis almost certainly due to a Covid-19 vaccine and clinically looked somewhat similar to an occlusion MI, so I got an immediate heart cath – Zero disease at all - totally clean.
So if I presumed I had disease based on the CT Cardiac Calcium, I’d be more aggressive with my lipids and also more worried I had disease … when I had none.
We’ve also seen the converse, a CT Cardiac Calcium that is minimal with significant Coronary Artery Disease.
It’s a nice screening tool - but doesn’t actually answer the question of whether someone has CAD.
As to the point on why bother, as the “evidence” is that stenting preventatively isn’t helpful.
I don’t think we really have a study showing this, under these circumstances. I see a fair number of people with occlusion myocardial infarctions - their CTCA the month before would have shown what? Take this group and act vs observe and see what happens.
The challenge is that only 25-30% of MI’s are due to major lesions – would you be happy with a 95% lesion in your LAD or RCA with conservative management … I’d not. But without a CTCA or a heart cath you’ll not know this.
The problem is scattered disease which with plaque rupture is 70% of MI’s - and this - yes I’d not push for a stent, but we’d be much more aggressive on lipid management and advise aspirin.
@DrFraser sorry to be repetitive but I think you missed part of my earlier question.
It seems you said a lot of calcium will interfere with some of the readings, but I think you notice a clear enough result that it will show you want you need to see, correct?
Just yesterday, my brother’s cardiologist said to get a nuclear stress test instead for this reason.
And my second question is when would you want someone to get a nuclear stress test vs a CCTA. I’m not clear on the differences. I had one 3 years ago. Does it show all the soft plaque but only not the lesions? Is CCTA always better? Do you feel both are good to do? Or partially redundant? Thank you.
If it’s stents we’re talking about they do prevent heart attacks and such when used as they typically do (mostly ACS). Avi did a meta analytic review when debunking Dr. Michael Greger et al on this.
My understanding is that stents provide symptom relief but have no statistical relevance in preventing heart attacks or reducing all-cause mortality.
“While stents are effective in reducing restenosis and the need for repeat revascularization procedures, they do not significantly reduce the incidence of heart attacks. Studies have shown that there is no significant difference in the rates of myocardial infarction between patients treated with stents and those undergoing percutaneous transluminal coronary angioplasty.”
“Compared with standard PTCAs, stents more often prevent restenosis and avoid the need for repeated procedures; however, they do not improve survival or prevent heart attacks. Using stents routinely rather than provisionally has only modest benefits.”
"The trials included 9918 patients with CHD. How was the study done? The researchers searched the medical literature to find randomized trials that compared coronary stents with PTCA. They found 29 trials that 1) included patients with CHD but no acute heart attack and 2) followed patients for at least 6 months after their procedure. In many trials, patients who had standard PTCA could have a stent if they developed complications or if the PTCA was unsuccessful. This bailout strategy was called provisional stenting. The researchers compared outcomes between groups by using special methods of analysis (meta-analysis). What did the researchers find? The researchers found no differences in numbers of heart attacks, coronary artery bypass surgeries, or deaths between groups. "
And you choose to ignore the error bars of your image.
Argue all you want, my take is that stents preventing heart attacks is not statistically
significant.
End of discussion.
Three of the studies were significant, and we look at the total sum which were.
A recent study published last year showing clear benefit of stents:
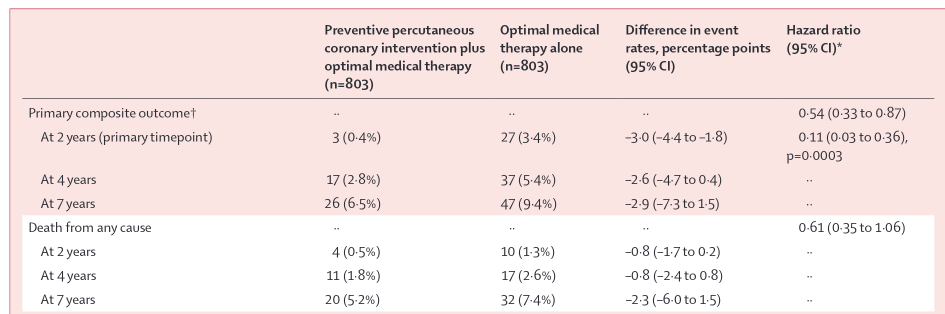
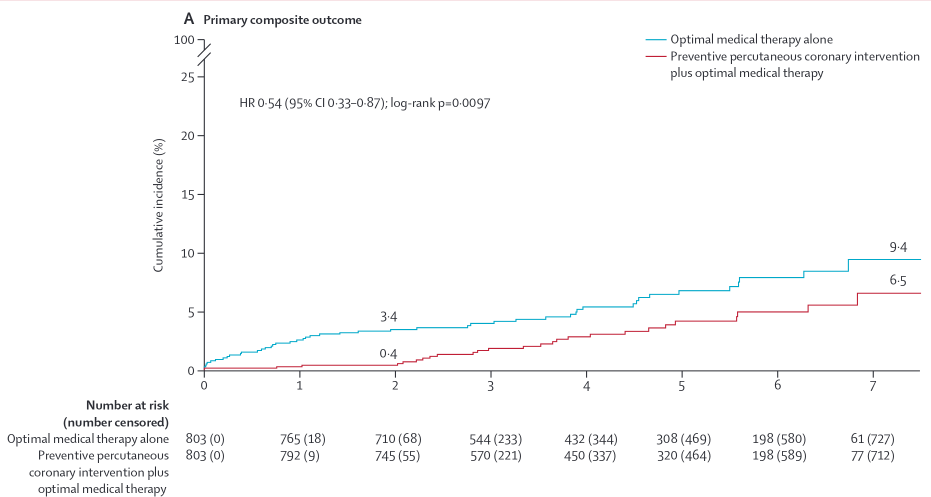
Between Sept 23, 2015, and Sept 29, 2021, 5627 patients were screened for eligibility, 1606 of whom were enrolled and randomly assigned to percutaneous coronary intervention (n=803) or optimal medical therapy alone (n=803). 1177 (73%) patients were men and 429 (27%) were women. 2-year follow-up for the primary outcome assessment was completed in 1556 (97%) patients (percutaneous coronary intervention group n=780; optimal medical therapy group n=776). At 2 years, the primary outcome occurred in three (0·4%) patients in the percutaneous coronary intervention group and in 27 (3·4%) patients in the medical therapy group (absolute difference –3·0 percentage points [95% CI –4·4 to –1·8]; p=0·0003).
Simply reducing events by 89% not bad, and this was also for vulnerable non-flow limiting plaque, trending to a decrease in all-cause death by 40% as well @relaxedmeatball thoughts?
This is why I find this all so confusing because I have not found a cardiologist (out of only 5) that said they would do a preventative stent, no matter what they saw on a CCTA . @DrFraser says the good ones do and I believe him. I am hoping he answers when you do a CCTA vs a nuclear stress test or vice versa…
Sorry, I’m not a cardiologist so I really don’t know about the benefits of stenting vs not. Hopefully I never need to find out first hand!
Generally I’m familiar with what @desertshores is saying about symptom relief but no difference in MI/deaths, but that’s not a strongly held belief. That said, symptom relief is still a pretty worthy goal IMO. And, as you said, maybe the better stent technology would translate into reduced MIs, which does seem very plausible.
Also this, with reservation I haven’t looked at this carefully nor really know much about this:
The meta analysis compared coronary stents with PTCA (standard balloon angioplasty), not medical therapy alone which is what most people do when not doing stents.
So in that study, stents with balloon angioplasty didn’t detect a statistically significant difference compared with balloon angioplasty on its own, but it looks like there was a non-significant trend towards reduced death by 30% for the one including stenting:
Few patients died in either group (65 [1.2%] for the PTCA group; 39 [0.8%] for the stent group). The odds ratio for death was 0.69 (95% CrI, 0.43 to 1.05).
So in this study no difference between balloon angioplasty (PTCA) and that with stent, correct?
However if we look at a more recent study with drug eluting stents (as that didn’t have), and that compared to medical therapy alone.
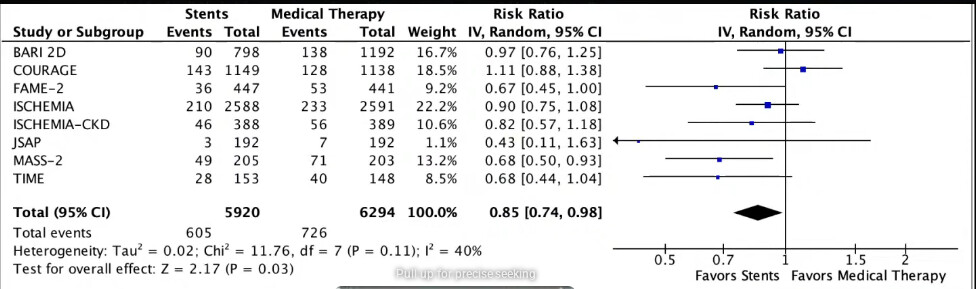
We can see that stents in contemporary trials reduce heart attack rates by 11%, while non-stent trials hasn’t detected a reduction in heart attacks at all (this is the balloon angioplasty etc), where there even was a trend towards increase in heart attacks.
However, the estimates favored revascularization (RR, 0.89 [95% CI, 0.80–0.998]; P=0.05) in the more contemporary stent-era trials, whereas in the older non–stent-era trials, the estimates favored initial medical therapy (RR, 1.42 [95% CI, 0.97–2.07]; P=0.07)
So we can at least say that compared to medical therapy only, stents reduce heart attacks.
I didn’t read that trial carefully, but what I thought would be interesting is they used some specific methods to detect and find vulnerable plaque that was also non-flow limiting. That appears to me plaque that doesn’t cause heart pain?
I was thinking maybe this trial is worthwhile to investigate further and if good investigate if it matters for those who have a lot of plaque and relevant plaque, thus stenting (and replicating the method), for whatever benefits that might entail.
So the study basically found vulnerable plaque that might rupture, and stented it, and it seems found massive benefits?
Seem like obvious in hindsight if so, find vulnerable plaque that might rupture, and place a mesh on it, but I don’t know either…