Interesting only one study in the meta analysis looking at bladder cancer risk in people using pioglitazone. However it was highly elevated risk of 14 events / 2605 vs control group of 6 events / 2633 and OR of 2.37. But to me it is suspect since it is a relatively small study and the bladder cancer incidence in controls is 3 x higher than other studies just glancing over the list. To me this suggest there may be confounding factors in the population they studied.
Also you have an occasional outlier SGLT2i study showing increased risk but when combined with the other studies the differences average out. OR ranges are huge for the majority of studies meaning the sample sizes need to be much larger to really get a meaningful answer since in most studies the range crosses the 1.0 mark.
Hence the meta analysis that in this case is quite useful and convincing. Makes me wonder about the pioglitazone data. I’d love to see a huge meta on pio like this but it seems people have generally stopped using it since the prevailing view is that it slightly increases the risk of bladder CA.
I discovered that I needed to drink a lot more water with Empa. Not quite as bad with Dapa.
It’s hard to change lifetime hydration habits.
There are quite a few studies that show bad things correlated with sodium over 141 mmol/L.
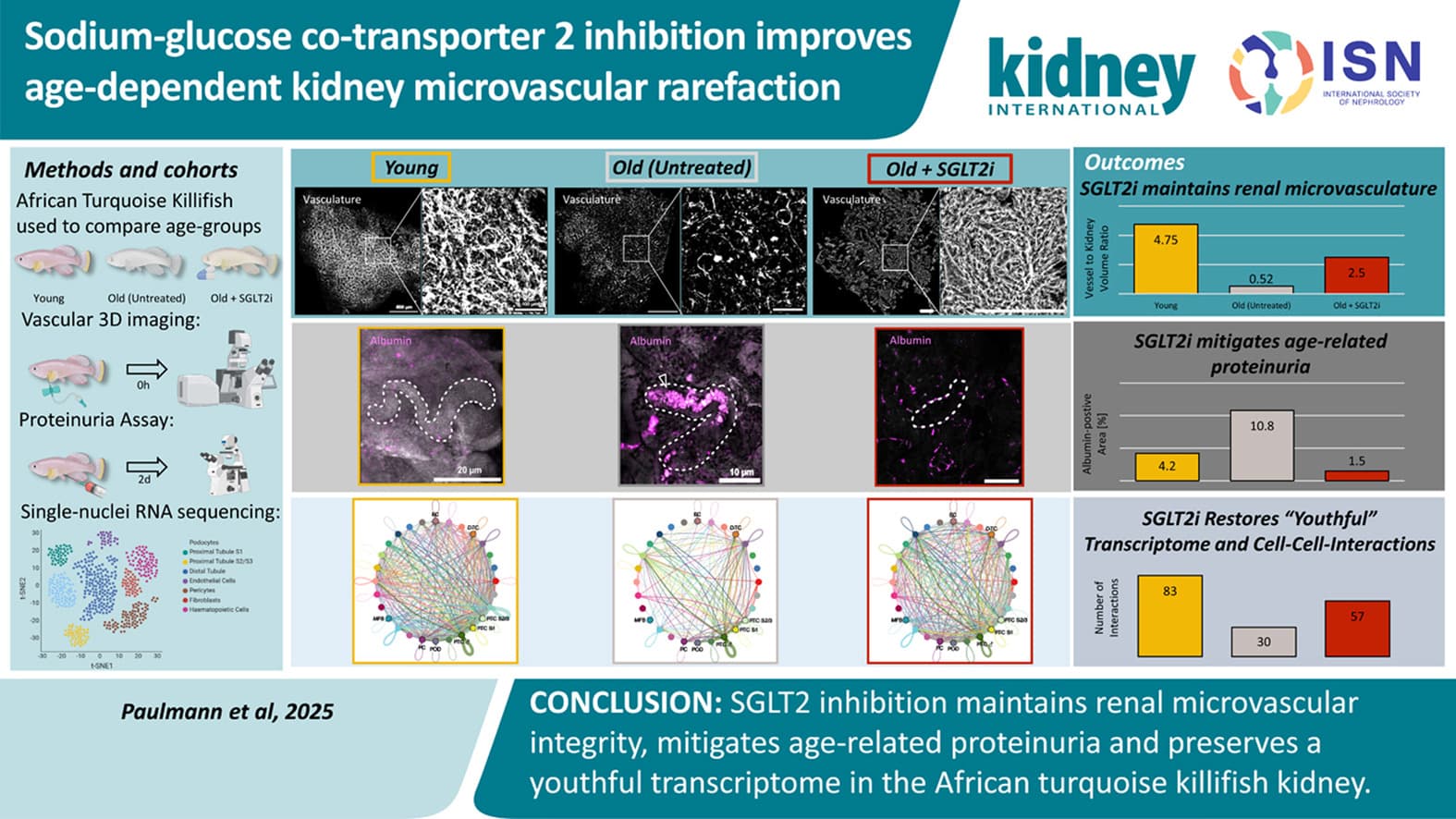
Our study establishes the killifish as a translational model for investigating kidney vascular aging. SGLT2i preserves kidney microvascular structure and function, reduces proteinuria, and maintains a more youthful transcriptome. These results support a vascular-protective role of SGLT2i in mitigating age-related kidney deterioration.
Is there an indication as to the definition of low dose? It is probably the lowest in the recommended range. I’m taking half of the minimum recommended dose of Canagliflozin and would like to see if there is any research on it. My BG was already within the normal range. I’m taking it primarily to slow the standard rate that even healthy kidney function declines. In that regard Canagliflozin and Telmisartan form functional reno-protective bookends.
Out of curiosity why Telmisartan and not Captopril? Reason I ask is because in the longevity data sheet that @Rapadmin had posted Captopril showed excellent results in middle age and while somehow reduced still good effects at old age also. Plus, it specifically says " Captopril is an ACE inhibitor used to treat high blood pressure, heart failure, “kidney disease”, and heart attack recovery.
Good question. My judgment is that Telmisartan has a more favorable benefit/side-effect/risk profile than Captopril and has a broader range of secondary benefits, especially for older adults. In addition, Captopril is cleared by the kidneys whereas Telmisartan is cleared by the liver, so there are considerations there, and Telmisartan has a significant and direct impact on the rate at which kidney function declines. Also important is the difference in half life and required dosage interval to prevent BP spikes (24 hours v. 1.9 hours). It is why Captopril is most often used in hospital and controlled environment settings.
I used jardiance for 2 years after metformin was giving me GI problems. My bloodwork was great but this past year started experience muscle cramping. Tried the usual - hydration, electrolytes, etc. Only thing that worked was stopping Empagliflozin. Anyone else experience this?
Been using it for past year at 1/3 of 25MG per day. No issue with muscle cramps, nor any other side effects I can tell. I do take Metformin between 500-1000mg daily also. I had bought a delayed release 1000mg metformin and every time I use it before bed, I tend to wake up more refreshened for some reason. I do crave sweets at times but that is the only bad/side effect I’ve noticed.
I also have more cramps but I thought it was more statin related rather than Empagloflizin, as I started both at the same time, but it’s an interesting point to consider.
No. not really. It is somewhat small and I just cut them approximately in 1/3’s. Obviously maybe one portion is 7.5mg, one 9mg and the other 8.5mg but I don’t think it matters that much. I just use a sharp pocket knife. As @Davin8r mentioned above cutting it in 1/2 is more practical and I have lately started taking 1/2 after taking 1/3rd for over a year.
I’m going to take it mostly for preservation of kidney function but also because I have been sitting on the border of pre-diabetic for a decade or more. On the other hand, I do not want to experience the possible symptoms. it isn’t worth it. Have you experienced any at the 8 mg dose?
Do you mean side effects from empagliflozin? If so, which side effects are you concerned about? These are very well-tolerated medications, especially in men.
UTIs aren’t something I personally even worry about from empagliflozin.
However, certain factors increase UTI risk in SGLT2 inhibitor users. Higher doses of dapagliflozin (10 mg) showed increased UTI risk compared to placebo (RR 1.23; 95% CI 1.03-1.46).[1] A 2023 meta-analysis confirmed that dapagliflozin 10 mg/day for >24 weeks was associated with significantly higher UTI risk (OR 1.27; 95% CI 1.13-1.43).[3] Additional risk factors include age ≥65 years, eGFR ≤60 mL/min/1.73 m², proteinuria, poor glycemic control, and diabetic microvascular complications.[1]
Severe UTIs remain rare across all SGLT2 inhibitors, with incidence consistently <2% in cardiovascular outcome trials. Meta-analyses showed no difference between SGLT2 inhibitors and controls for pyelonephritis (RR 0.78; 95% CI 0.52-1.18) or urosepsis.[1][4]
Importantly, a 2025 study found that discontinuing SGLT2 inhibitors after a UTI was associated with higher cardiovascular and renal risks (HR 1.35 for both) without reducing recurrent UTI risk (HR 0.96; 95% CI 0.22-4.29), suggesting continuation is generally appropriate.
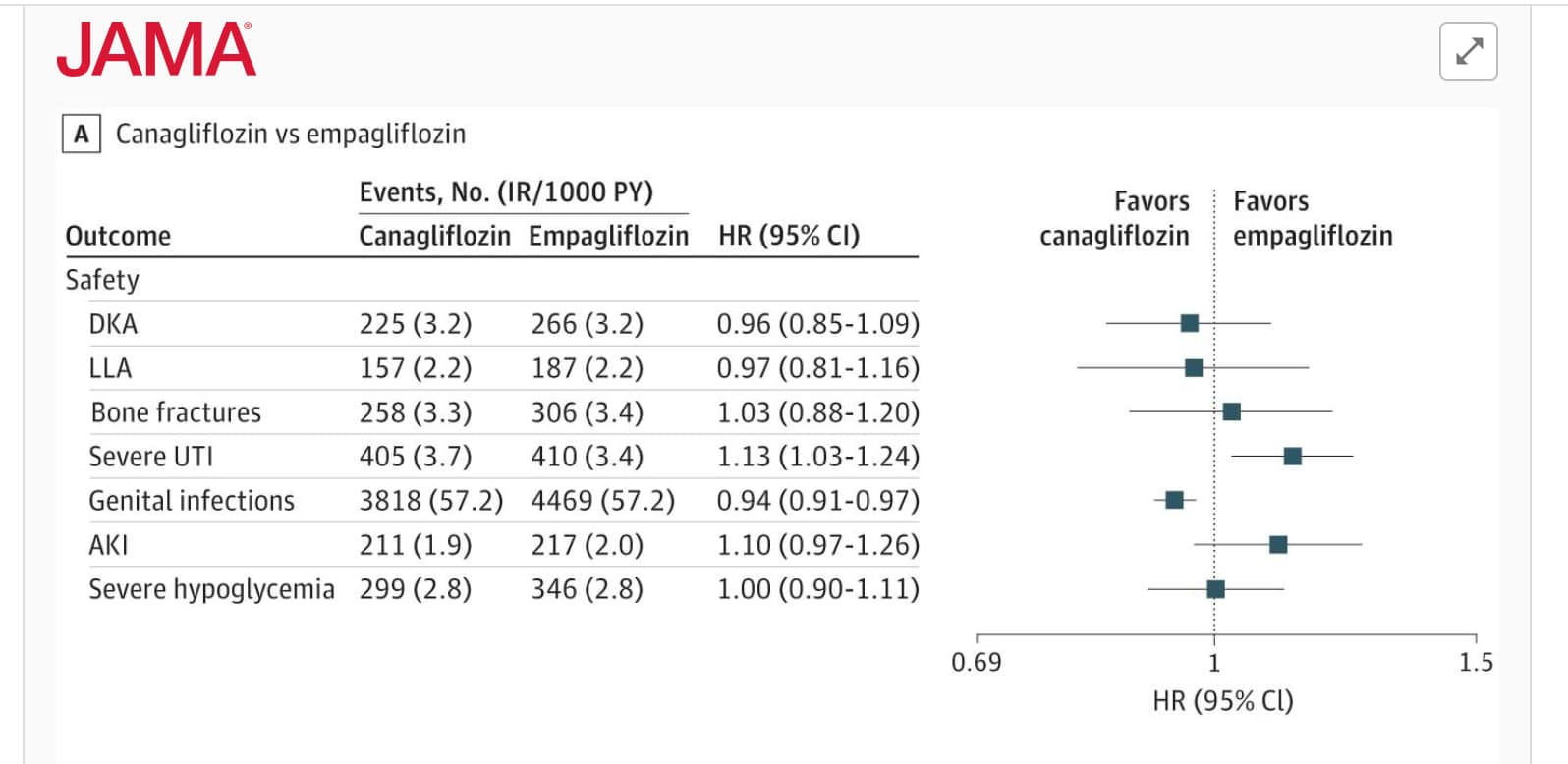
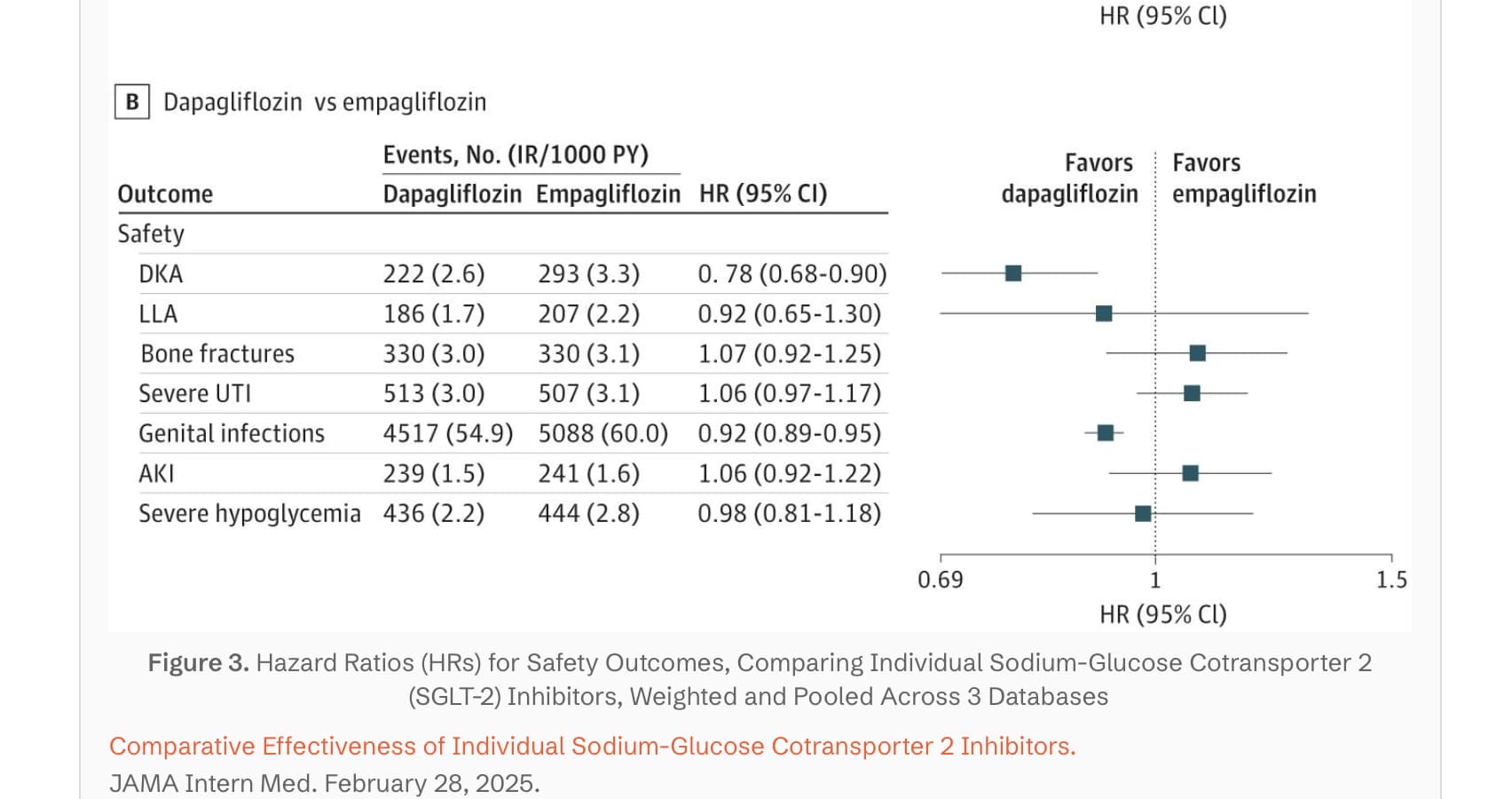
This comparative safety analysis shows that severe UTI risk is generally comparable across individual SGLT2 inhibitors, though canagliflozin demonstrates a modestly higher risk compared to empagliflozin, while dapagliflozin shows similar rates.
I don’t believe the rates of UTI with empagliflozin in men differ from a placebo. What is slightly increased are the rates of genital fungi infections, although the rates are minimally elevated in those who do not have diabetes and are circumcised. Overall it is not a concern for me (25mg/day empa), although I have purchased a bunch of microbe testing urine strips, and use one approximately once a month to catch any possible asymptomatic infection. I’ve been on empa for over a year, and no issues so far.