I would really like to know how these drugs are meant to achieve all the claimed effects. As far as I know, SGLT2 is mostly expressed in the nephrons of the kidneys. In this case it would be reasonable (IMO) to believe that the effects factor through the antidiabetic action. But how likely is this?
Perhaps there’s a hormone from the body of the kidney?
There are other SGLT isoforms (beyond 1 and 2) that are poorly understood, as far as a brief search shows. Some of those are more widely expressed in the body.
Or could there be an entirely separate mechanism of action?
Yes, but also expressed (albeit at lower levels) in heart cells (cardiomyocytes) and endothelial cells of blood vessels. Current theory is that biding of SGLT2i to these receptors plays a major role in these drugs’ action on CVD.
That always raises the question in my mind of to what degree those drugs work only in the context of a pathological state. If you have heart failure or whatnot, the drug will ameliorate some of the damaging factors in heart failure. But perhaps the drug will be at best neutral in a healthy heart, because those pathological factors are not present. If it is raining huge baseball size ice, wearing a helmet makes your health better, but if it is sunny and mild outside, the helmet only makes you hot. Many here (most?) don’t take SGLT2i drugs because they’re diabetic, have heart or kidney issues. Do they still benefit overall at an acceptable side effects cost? For understandable reasons medication studies are in sick people, not healthy, so trying to figure out reliably what happens in healthy humans is tough. What we have left is mice and canagliflozin in ITP.
Great paper! I’ll have to study it more carefully.
Nevertheless, it remains uncertain whether all SGLT2 inhibitors share the same class of effects including their off-target cardioprotective abilities and the specific patient populations that benefit most. Some meta-analyses have compared the effects of SGLT2 inhibitors in specific populations, but debates persist. For example, while some clinical trials suggested that EMPA offers greater CV protection than CANA and DAPA in diabetic patients, others have not found significant differences between these drugs. Despite increasing evidence of the cardioprotective benefits of SGLT2 inhibitors, there is still limited data comparing these agents in nondiabetic patients and those with HFrEF or HFpEF. Therefore, further research in these specific populations is needed.
83/96 patients completed the study (age 68.7±8.9 years, 73.5% males, GFR 49±17 ml/min/1.73m2, median albuminuria: 0.18 [IQR 0.10-0.38] g/24h). After 12 weeks of dapagliflozin, nighttime SBP declined by -3.0 mmHg (95%CI -5.2/-0.8 mmHg; P=0.010) with an improvement of nighttime SBP goal (<110 mmHg) from 18.0% to 27.0% (P<0.001). Similarly, the prevalence of normal dipping increased (from 31.3% to 50.6 %, P=0.005). A decrease in daytime (-2.4 mmHg; P=0.046) and office (-7.9 mmHg; P=0.009) SBP was also found. The decline of ambulatory and office SBP was associated with increased prevalence of CH (from 6.0% to 18.0%) and significant improvement of SH, WCH and MH (P=0.009). Albuminuria decreased (P<0.001) whereas eGFR did not change (p=0.297). Urinary tract infection (4.2%) and acute kidney injury (3.6%) were the main causes of drop-out. Only one patient showed a drop of nighttime SBP below 90 mmHg.
I haven’t jumped through the hoops to access this yet. Do they actually claim to measure the transporter expression in these cells? I know some groups have claims along these lines (on the m-rna level).
Skimming the paper it seems their mechanism is plausibly downstream of the antidiabetic effects?
Here’s a recent paper giving modest evidence that the endothelial effects are due to inhibiting other sodium-stuff co-transporters:
In patients with T2D, the cardiorenal benefits of treatment with SGLT2-Is and GLP1-RAs were similar in patients with normal baseline BP compared to those with a higher baseline BP.
Important result. Any time there’s a study with an important biomarker within healthy range and the effect of a drug like SGLT2i or GLP-1RA showing good effect - rather than only working in impaired subjects - that’s good news for those of us who are healthy (at least in this respect), who still want to derive benefits from taking these drugs.
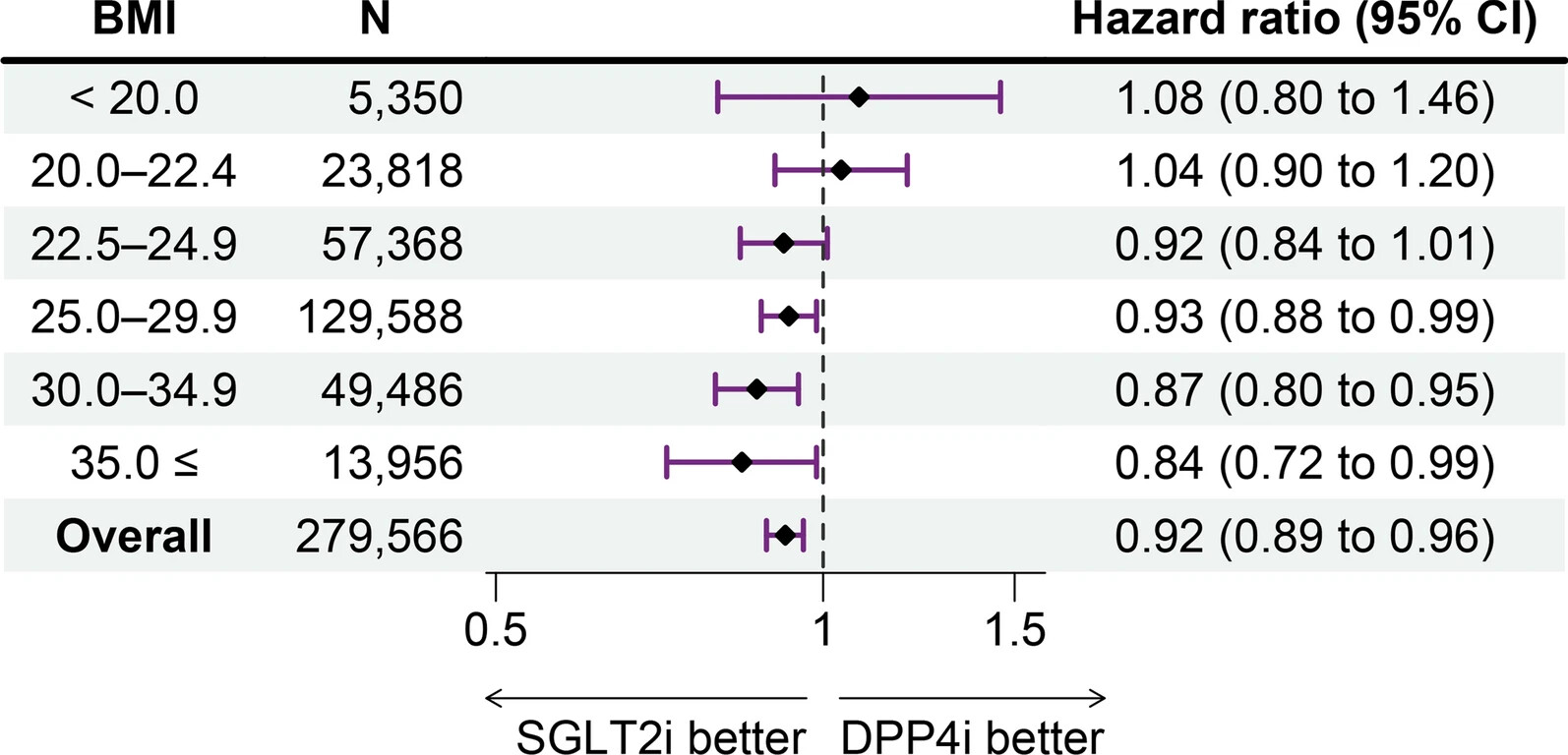
The protective effect of SGLT2 inhibitors on cardiovascular events among patients with type 2 diabetes appeared to decrease with lower BMI and was not significant among patients with low-to-normal BMI (< 25.0 kg/m2). These findings suggest the importance of considering BMI when initiating SGLT2 inhibitors.
Isn’t the hazard ratio for the comparison between SGLT2i and DPP4i?
As in, for lower BMIs, DPP4i may reduce CVD events more than SGLT2i, but SGLT2i might still reduce CVD events?
You’re right, but DPP4i are not cardioprotective as far as I know. That’s why association studies often use them as the comparator. Still your point stands: we should look at RCT results stratified by BMI.
There were significantly fewer hospitalizations for HF (OR: 0.70, 95%CI: 0.64–0.76), cardiovascular deaths (OR:0.86, 95%CI: 0.77–0.97) and all-cause deaths (OR:0.90, 95%CI: 0.82–0.98) in the SGLT2 inhibitors group compared to the placebo group, without any interaction with BMI group (test for subgroup differences: x2 = 1.79, p = 0.62; x2 = 0.27, p = 0.97; x2 = 0.39, p = 0.94, respectively). There is no interaction between the efficacy of SGLT2 inhibitors and BMI in patients with HF with either preserved or reduced ejection fraction. SGLT2 inhibitors are associated with improved outcomes regardless of the BMI.
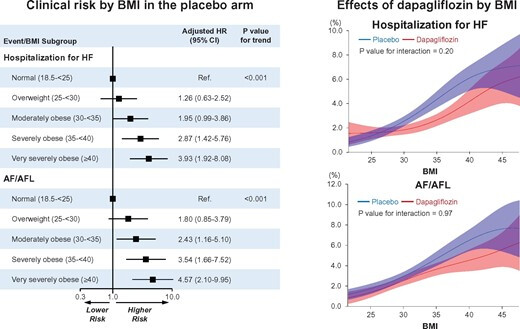
Although relative risk reductions in CV and renal-specific composite outcomes with dapagliflozin did not significantly differ across the range of BMI (P for interaction ≥0.20 for all outcomes), obese patients (BMI ≥ 30 kg/m2) tended to derive greater absolute risk reduction in HHF and AF/AFL (P for interaction 0.02 and 0.09, respectively) than non-obese patients.
Doesn’t that appear to say that empagliflozin is slightly more protective at lower BMI compared to dapagliflozin? Still, the heterogenous results across different studies give onne pause. Regarding the comparison to DPP4i, first, note they actively excluded those without diabetes - perhaps people who have diabetes at low BMI are different from those who have diabetes at higher BMI. Second, in that study, they don’t appear to break out the individual SGLT2i, and if one were to take the second study at face value, there may be subtle differences in outcome among them.
However, there is another disturbing signal, not mentioned by adssx, and that is that the results of SGLT2i treatment were particularly bad (compared to DPP4i) for those patients who were 60 or older - this jumped out at me, as I’m 66, and was unremarked upon by adssx, because he is much younger and possibly doesn’t plan on reaching such a deprecated age, preferring to stay eternally young
But seriously, we need rcts that go by age, bmi, and different SGLT2i, as that above 60 signal is very strong, and disturbing.
They’re not particularly bad. You should check RCTs and subanalyses by age but I think everything is okay. Stratification by age is a standard analysis done by researchers, companies, and regulators (same for gender). I’ve never read anything about SGLT2i being less effective among people > 60yo.
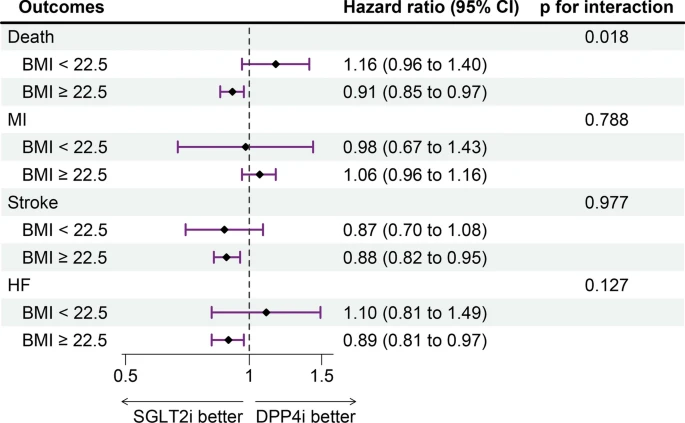
Look at figure 4. What do you mean, not particularly bad? And in the text above the figure 4 they say so themselves.
“In the subgroup analysis, we observed the consistent trends of the heterogeneity by BMI category (i.e., < 22.5 kg/m2 vs. ≥ 22.5 kg/m2) particularly among adults aged ≥ 60 years[emph. mine CT] (HR [95% CI] in BMI < 22.5 vs. ≥ 22.5 kg/m2, 1.14 [0.96 to 1.35] vs. 0.96 [0.90 to 1.03]; p-for-interaction = 0.052), among male (1.06 [0.93 to 1.21] vs. 0.91 [0.87 to 0.95]; p-for-interaction = 0.019), and among prevalent users of DPP4 inhibitors (1.06 [0.92 to 1.23] vs. 0.93 [0.89 to 0.98]; p-for-interaction = 0.054) (Fig. 4).”
Again, it must be emphasized that this population might have a different outcome to low-normal BMI above 60yo, who are not diabetic and take rapamycin concurrently. And, FWIW, in the ITP the mice on cana didn’t die earlier.
No, it’s in comparison to DPP4i. That’s what figure 4 shows. SGLT2i have drastically greater hazard ratios for 60+yo, compared to DPP4i users (i.e. general population, since DPP4i are neutral in theses outcomes).