Yeah, but you would need to do trials on humans at different ages with different levels of nutrients. All the nutrients. And the humans have different DNA, so at this point the totality of evidence amounts to around zero.
Feeding animals in confinement, like we do pigs, gives very useful information. They are in a closed room on a concrete or plastic slatted floor (so the poop can get away) and eating only what is in the feed. It took years to get this right, but I have to admit they’re really efficient now. Not optimized for longevity, but really efficient.
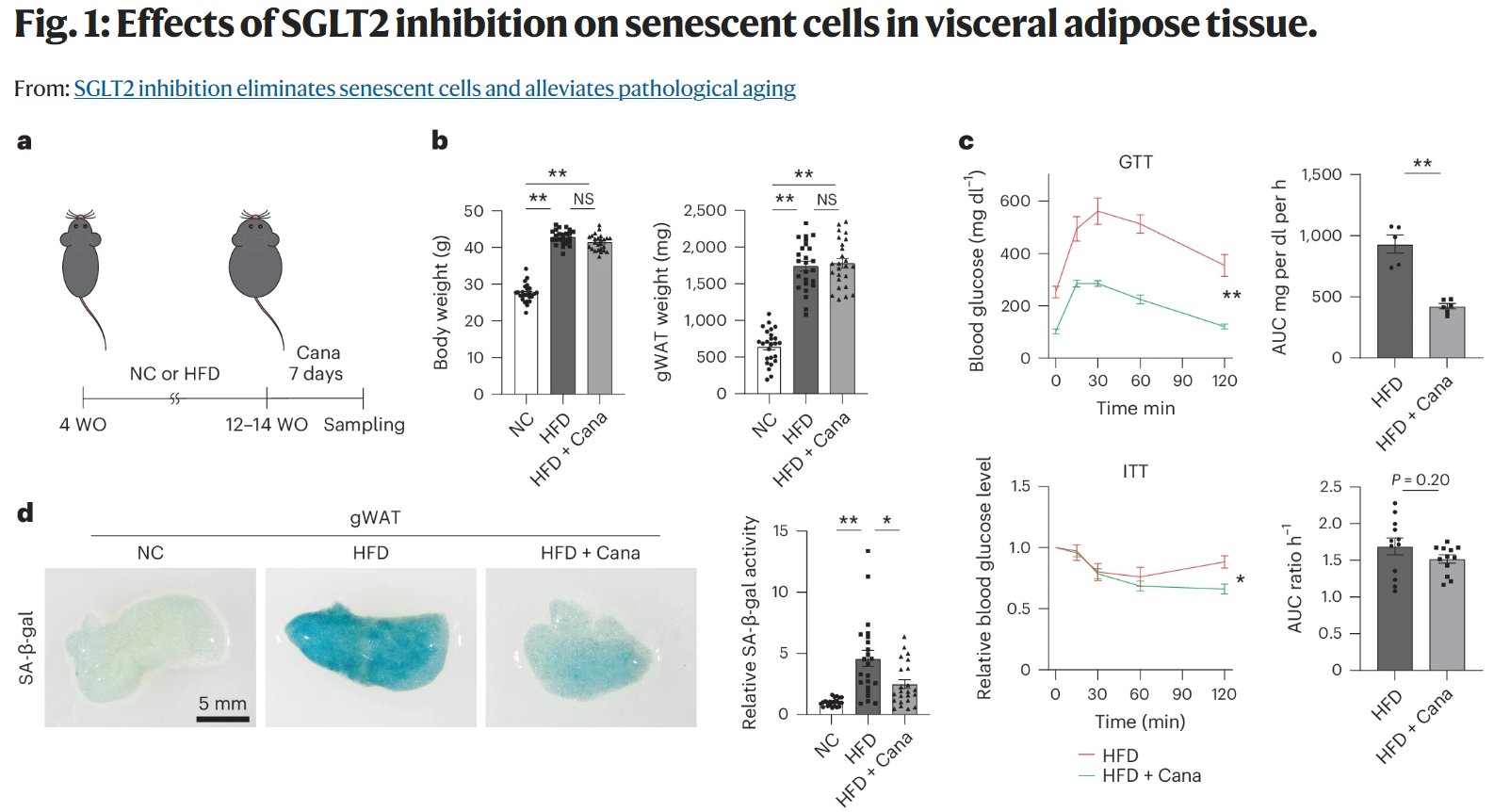
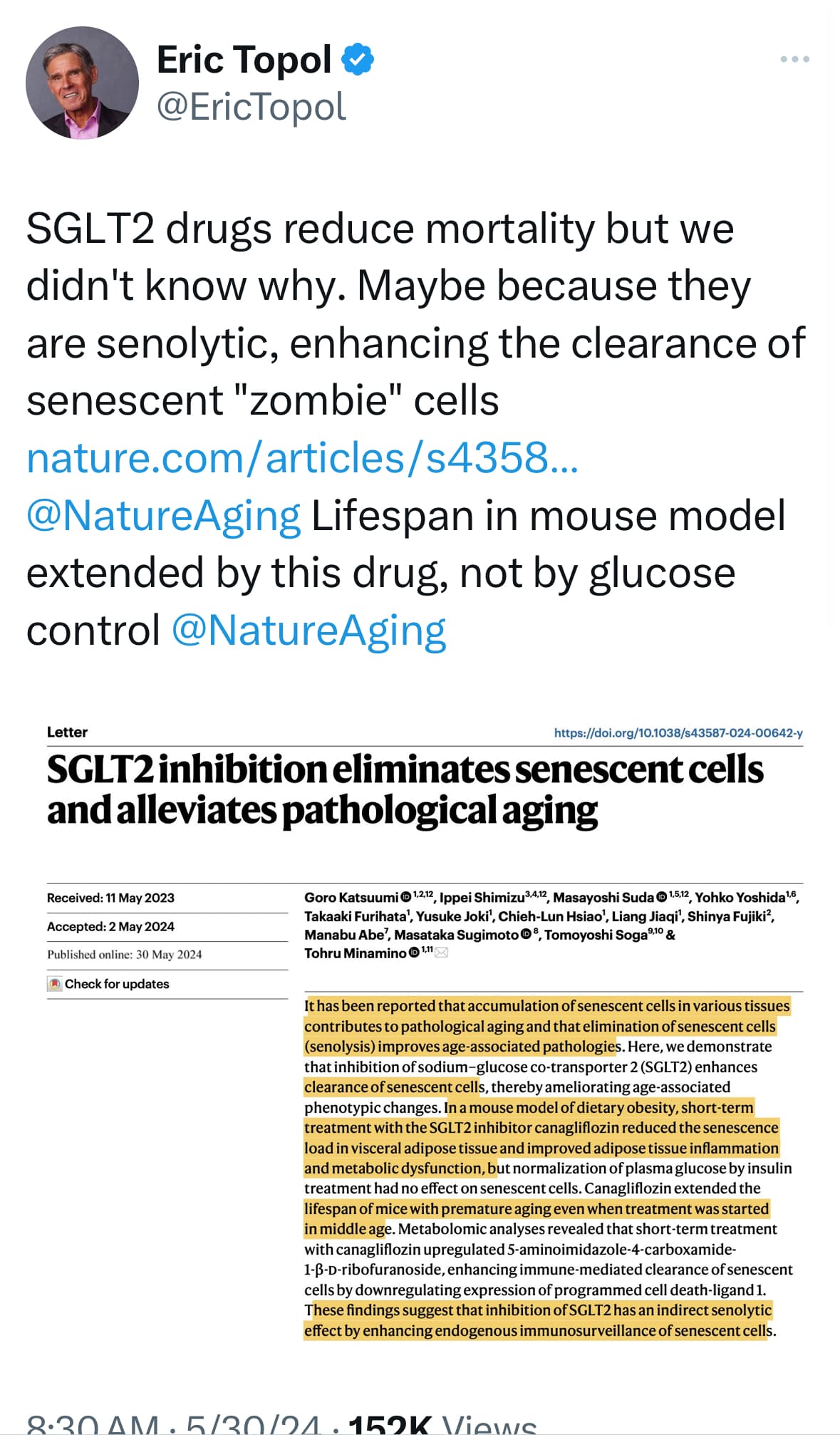
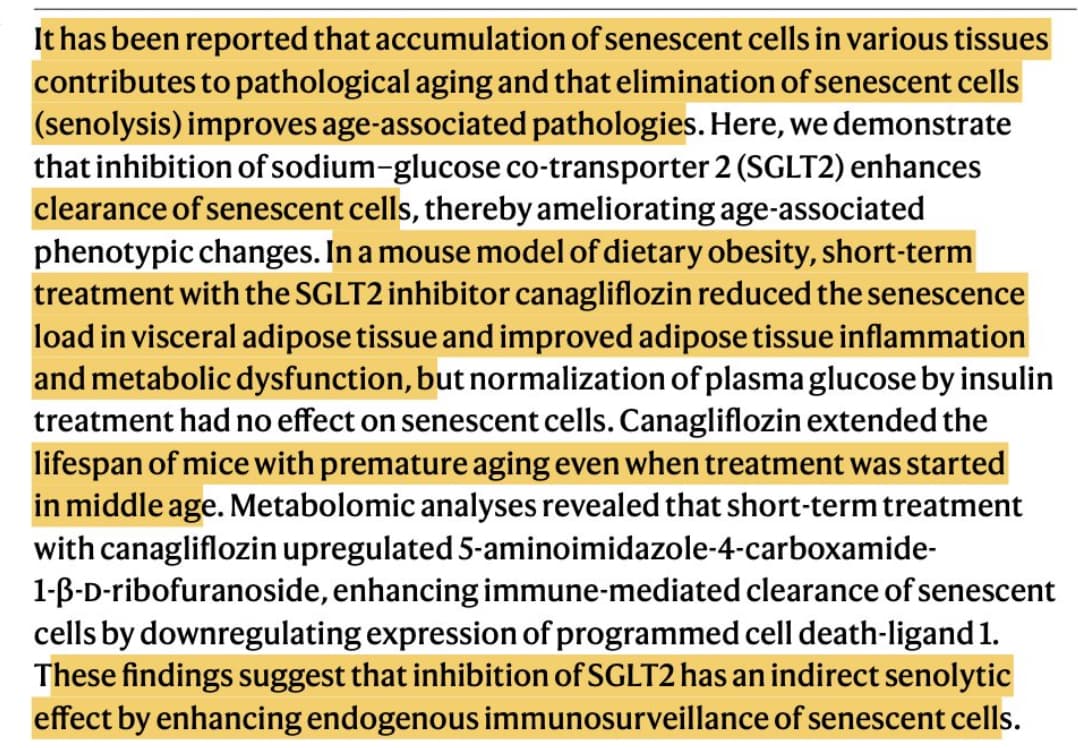
“In this paper, researchers have found in male mice that SGLT2 inhibitors, used to treat diabetes, “reduced the senescence load in visceral adipose tissue and improved adipose tissue inflammation and metabolic dysfunction”.
Unless I misunderstood, the paper does not prove that SGLT2 inhibition “eliminates senescent cells and alleviates pathological aging”. It proves that canagliflozin does so. But it might be due to SGLT1 inhibition or to an off-target pathway. The only way to prove that it’s not SGLT1 inhibition would be to do the same study with empagliflozin (it could still be off-target, though).
(1) The formation of AS plaques in ApoE -/- mice showed a downward trend under DAPA. (2) After the intervention of Ang II, the cell activity of RAW264.7 decreased, and the expression of senescent cells and related genes increased. (3) Under the Ang II condition, the expression of SGLT2 and NHE1 increased, and SGLT2, NHE1, and senescence-related genes decreased with the addition of DAPA. (4) The expression of NHE1, senescent cells and related genes decreased in RAW264.7 cells after DAPA treatment with plasmid NHE1 intervention.
Dapagliflozin only has limited SGTL1 inhibition potency, so it’s most likely not SGLT1.
This also suggests a potential for additive/synergistic (or possibly just redundant) effect of angiotensin II inhibition (ARB or ACEi) in this process.
RAS blockade and SGLT2 inhibition display synergistic beneficial effects on BP, kidney injury and cardiac hypertrophy in a rat with hypertension and diabetes. The synergy does not involve upregulation of angiotensin-(1–7), but may relate to direct RAS-independent effects of empagliflozin in the heart and kidney.
Our study showed that SGLT2i may be safely used without increasing END after AIS. Remarkably, acute phase SGLT2i use was significantly associated with better neurological outcomes at 3 months, while acute outcomes at discharge were not affected. Continuing SGLT2i use beyond discharge, rather than transient use during admission, was associated with a more favorable 3-month functional outcome.
In conclusion, our findings suggest that SGLT2i may be a priority for diabetic patients with AIS because of its potential benefits on neurological outcomes.
I know why it reduces mortality besides the senolytic effect. High glucose in serum = fat gain = plaque buildup in arteries of the brain, kidneys, and heart. When I get a Urinalysis, it is with great pleasure that when I read the report, the excertion of glucose from my body is off the charts.
Our study is the first to compare before and after peak VO2 values of the OMT+SGLT2i group to the patient’s own baseline and we found no significant improvement.
SGLT2 inhibitors are the only ones that actually removes the glucose from the body continously all day long in the urine. Get a urinalysis and you will see the numbers off the chart.
For the first time we discovered that the SGLT2 inhibition may exert protection on bronchial and lung cancer and non-melanoma skin cancer from a genetic perspective. However, suggestive higher cancer risks of bladder, prostate, and corpus uteri were also noted, which warrants real-world data validation in the future.