The vast majority of their positive effects are glucose-independent. That’s why SGLT2is are approved in CKD and HF, contrary to other antidiabetic drugs (and they might be extended to NAFLD and HCM). And that’s also why they protect more from AD and dementia than other anti-diabetic drugs. See here for some overviews: Acarbose - Details On Another Top Anti-Aging Drug - #448 by adssx
Looking at those diagrams, though – don’t they all start with glycosuria? One points out increased sodium excretion as well. All the other beneficial effects appear to be downstream, don’t they? If this is the case, couldn’t we get these same downstream benefits by simply eating less sodium and sugar?
(Note I don’t want the above to be true. I take empagliflozin and I want to believe this med is useful!)
The diagrams are, of course, simplifications. And we cannot draw what we don’t know: we know that the benefits are largely glucose-independent (as other antidiabetic drugs don’t do as well and as the benefits are independent from baseline Hb A1c and Hb A1c reduction). The articles say:
“These benefits have been demonstrated in trials of SGLT2is, and appear, to some degree, to be independent of glycemia and substantial weight loss.”
“Otherwise stated, these agents have direct, glycosuria-independent, effects that decrease cellular stress and enhance cell survival.”
ACM divided by 2 vs metformin: Canagliflozin - Another Top Anti-aging Drug - #705 by adssx (see also the paper explaining their potential off-target mechanisms “including the inhibition of gut microbiome–mediated uremic toxin formation”)
So no, just reducing one’s sugar intake is not equivalent to taking SGLT2.
Yes that’s true, but it’s still possible those could be downstream effects. What I’m looking for is a mechanistic explanation that ties SGLT2 inhibition to all of these effects, other than glycosuria/natriuria. We don’t have that yet, do we?
Oh c’mon now. We have plenty of nice mechanistic data for all kinds of drugs. Look at rapamycin and mTOR! By knowing how things work, it opens up possibilities for other targets in the pathway(s) which may be even safer and/or more effective.
And I think that this doesn’t include drugs with additional unknown targets. Mechanistic theories are interesting, but in some situations, such as for SGLT2i, they’re useless.
That’s why Eric Schmidt funded EveBio to map all FDA-approved drugs and targets. They’ve told me they’ve already found some crazy results. The data will be published in open data later this year.
You’d still need clinical trials for those targets in the same pathways either way for it to be comparable. If you believe sodium or sugar restriction would have the same benefit, you can look up if such clinical trials exist.
Two smart people cannot agree to disagree so I won’t I said it’s useless here because we know that we don’t know. So expecting a mechanistic explanation is a waste of time. Of course, it would be nice to have one.
They compared dapagliflozin with “standard of care” (SOC, I assume, metformin and other non-SGLT2 antidiabetic drugs?) “in patients with type 2 diabetes free from cardiovascular disease”. Differences in HbA1c and insulin resistance (HOMA-IR) were nonsignificant (although close, p=0.09, over just 6 months). On the other hand, dapagliflozin, compared with SOC significantly:
Decreased weight (–1.5 kg)
Decreased BMI (–0.62)
Decreased SBP (–7.63 mmHg, poke @Davin8r, I was wrong; it looks like it decreases SBP even in normotensive non-obese people, at least with T2D: “The overall study population tended to be overweight, with a mean body mass index of 26.38±4.39 kg/m2 and a mean waist circumference of 92.53±11.13 cm. The baseline mean systolic and diastolic blood pressure was 130.24±13.89 and 76.36±11.09 mm Hg, respectively.”)
Increased hematocrit
Increased blood urea nitrogen
Dapagliflozin also produced beneficial effects on cardiac geometry and diverse mechanical properties via cardiac structural and functional remodeling: greater reduction in left ventricular (LV) dimension and LV mass index, LV global longitudinal strain increment and improved LV systolic and early diastolic strain rates.
They offer some potential mechanisms (and discard others):
These findings suggest that the favorable effects of SGLT2i on cardiac geometry may extend from patients with clinically evident HF to a population with preclinical diabetic cardiomyopathy.
While SGLT2 is believed to provide additional energy substrates that fuel the failing heart by facilitating a ketogenetic environment, it may also enhance cardiac energy use, resulting in a metabolic shift from glucose oxidation toward more effective fatty acid oxidation and improved mitochondrial function. Additional electromechanical cardiac benefits from SGLT2is may be mediated through improved cardiomyocytes ion channel transporters (eg, sodium‐hydrogen exchanger 1, Ca2+ handling, or late‐INa) function. Indeed, we observed significant improvement in GLS and systolic strain rate with a paralleled increment of diastolic strain rate after 24 weeks of dapagliflozin add‐on therapy compared with the conventional antidiabetic regimen.
Accumulating evidence suggests that SGLT2is may mediate cardioprotective benefits through anti‐inflammatory and antifibrotic effects. In our study, we hypothesized that 24 weeks of dapagliflozin add‐on therapy mitigated cardiac fibrosis by reducing proinflammatory mediators compared with the SOC group. However, we found no change in transforming growth factor‐β, tumor necrosis factor receptor 1, fatty acid–binding protein 4, growth differentiation factor 15, or hsCRP levels.
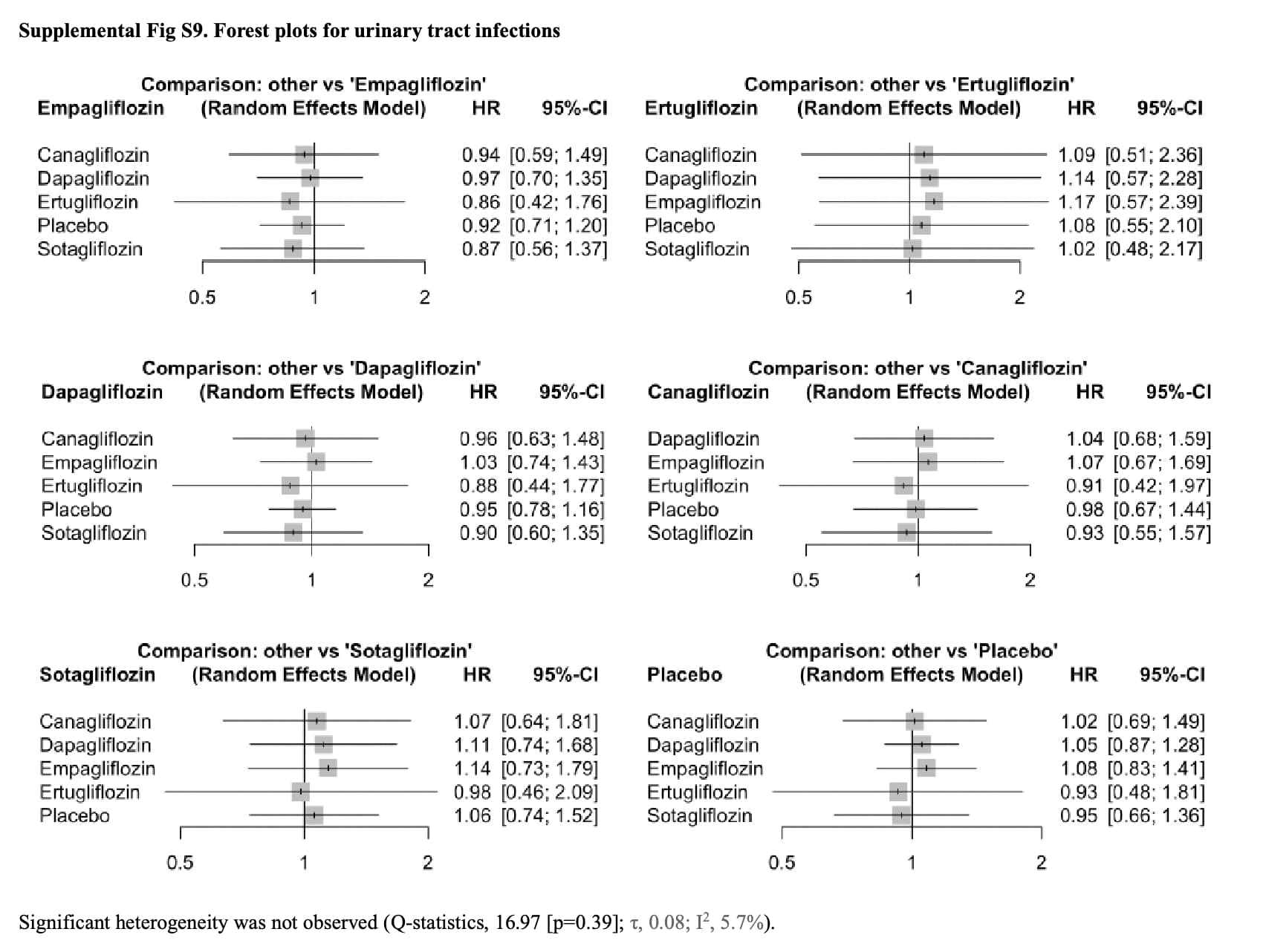
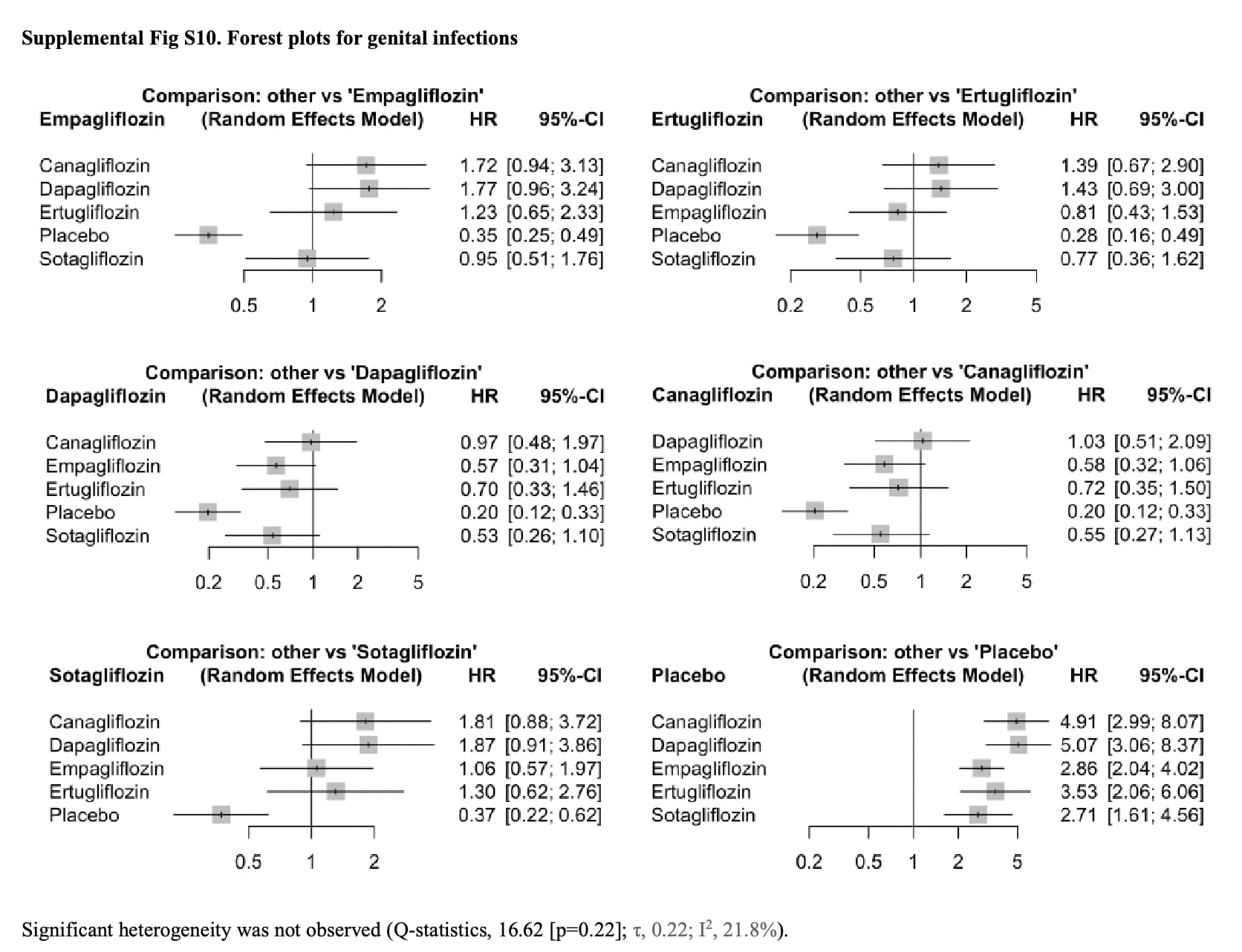
Since you’ve had multiple UTI’s it’s worth knowing it could increase risk for them, for you and your parents if there is a genetic component. In elderly especially it could result in delirium and confusion or worse of course. Elderly can also have a harder time to understand their own situation on average, so some might not be able to detect an UTI for example.
I forgot about that, but I’ll have to look closer to understand this more and what evidence was the reason for it’s been mentioned in the past if it was just observational trials (it’s a good story about glucose being a breeding ground for bacteria in the urinary tract, could influence things in an inaccurate way).