Ah those mice and the ITP…translation to humans is massive leap.
I didn’t find first glance, but my guess…curve will be SAME, just perhaps the delta shift might not be as much.
Ah those mice and the ITP…translation to humans is massive leap.
I didn’t find first glance, but my guess…curve will be SAME, just perhaps the delta shift might not be as much.
Yes - but what we are all betting on ![]()
Well thats’ new and pertinent information you’ve shared re risk calculus.
Do you have/use a CGM? Is anyone else of low BMI, far away from T2D using this med with a CGM?
Researching the issue of hypoglycemia for people using SGLT2 inhibitors a little more…
A study of 170,000 diabetic Japanese patients on SGLT2 inhibitors saw a risk of %0.13
So - in diabetic populations, around 1 in 1,000 patients.
But, the study notes:
Conclusions: …We revealed that the risk of hypoglycemia may be higher when combining SGLT2 inhibitors with sulfonylureas and/or insulin. Furthermore, we discovered a high risk of hypoglycemia in older and non-obese patients.
Yes - I reported on my results with Canagliflozin here, with CGM tracking screen shots (keep in mind that the real blood stick tests suggested the CGM was 10 to 20 points lower than the blood tests):
Diabetics? They have massive glucose stores, would naturally assume hypoglcemia would NEVER be a risk.
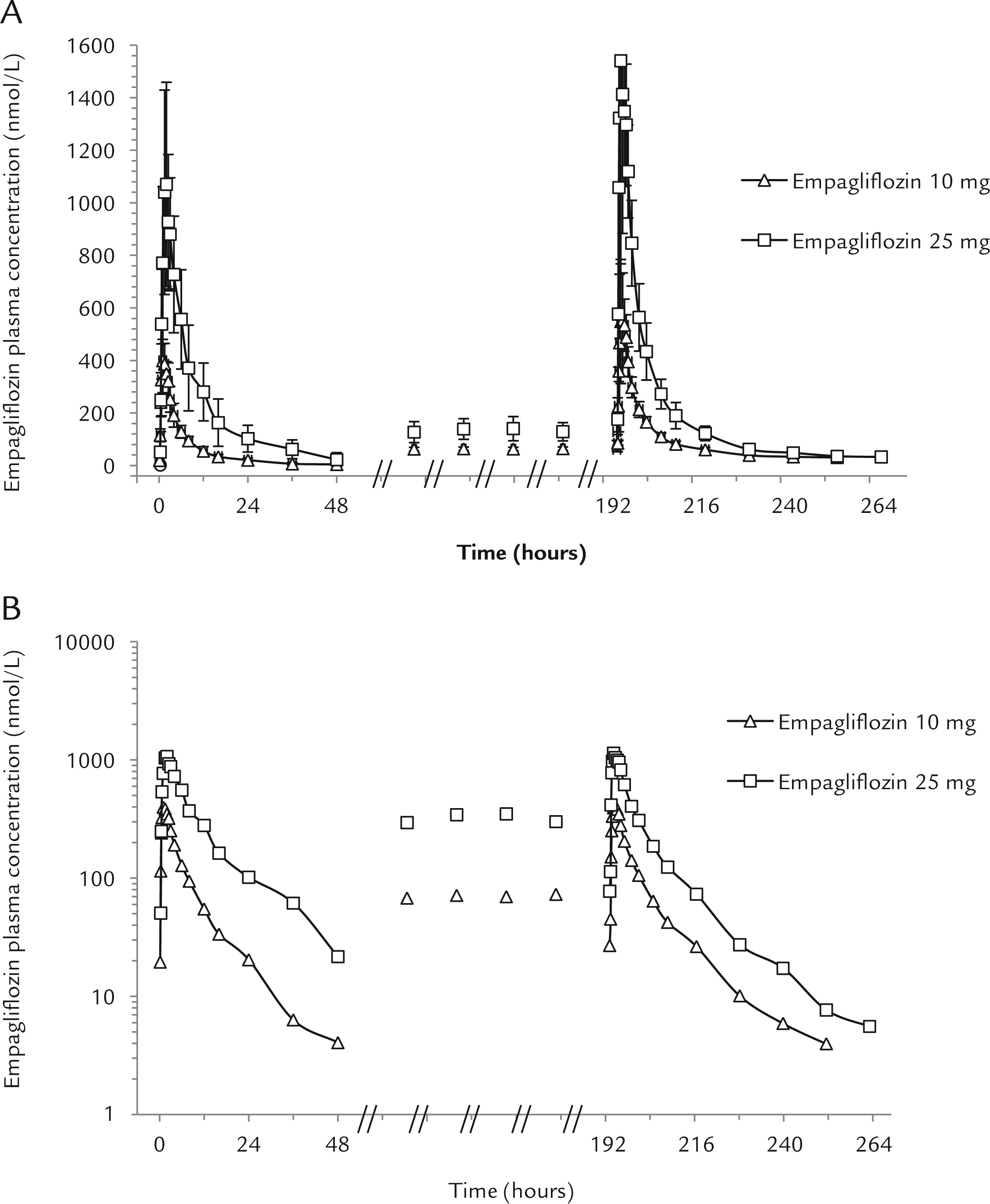
Looking at the curve above, using my fasting glucose and fasted state, along with pharmacokinetics, I’d be immediately and in a sustained hypoglycemic state taking10mg.
Anyone at any age can get Fournier’s gangrene with no past medical history. All you need is a skin breach from an insect bite or minor laceration/trauma.
The genital/peritoneum area is literally one of the worst possible place you can get necrotizing fasciitis (aka “flesh-eating” bacteria) besides head and neck
It’s rare for young and healthy people, but possible.
Men are about 10x more likely to get Fournier’s gangrene and especially if you have immunosuppression (i.e. high dose rapamycin on the first day leading to neutropenia) and canagliflozin - the risk skyrockets even further.
The main association is you can see it in a male T2DM (= some immunosuppression) patient using canagliflozin. But the problem is if you show up in the urgent care/ED and “your doctor is not really a doctor” and doesn’t think of urgent surgery and just sends you home with antibiotics…
Which SLGT2 are you taking nowadays, and any different side effects from previous?
Empagliflozin - no side effects that I can notice.
I would be willing to bet you take supplements or medications that are more dangerous than SGLT2 inhibitors.
The risk-reward ratio falls heavily on the side of canagliflozin and empagliflozin.
I do not understand your concern about these proven drugs. As I said before, aspirin is probably more dangerous.
" Risks should not be evaluated without considering attendant benefits."
"What causes Fournier’s gangrene?
Fournier’s gangrene can occur when a person has a skin wound that allows bacteria, viruses, or fungi to get deeper into the body. Examples of these skin injuries include anorectal abscesses, surgical incisions, diverticulitis, rectal cancer, or genital piercings."
"20 to 70 percent of those with Fournier’s gangrene have diabetes. An estimated 25 to 50 percent have an alcohol use disorder."
"About 1.6 out of 100,000 males will get Fournier’s gangrene"
“Fournier’s gangrene is a rare disease. Very few people with diabetes should get this bacterial infection.”
Fournier’s Gangrene: Causes, Symptoms, Diagnosis & Treatment.
This is only here because I quoted from it.
Please don’t use this forum as a tool to disparage NPs and PAs. Malpractice claim rates are far lower for PAs and NPs compared with physicians:
Anyone can make a bad decision (including a doctor), but it doesn’t mean the entire profession should be held accountable for it.
Is there an argument to be made for using Canagliflozen over Empagliflozin for our purposes?
As I’m understanding it, there’s a lot more research on Canagliflozin, which is its main positive. However the risk profile for Empagliflozin is better and the assumption is that Empagliflozin would have performed similarly. So, advantage: Empagliflozin. Correct?
I’m thinking it would be a good/logical approach to take an SGLT@ inhibitor, likely Empagliflozin, on a similar schedule as Rapamycin and, additionally, take acarbose prior to any medium/high carb meal? Is my thinking correct?
I’m new here and my head is kinda spinning for the wealth of information. I’ve been taking Metformin, but it seems that these are better options (I’m not T2D, btw).
I’m not looking to disparage all NPs nor am I saying physicians make no bad decisions.
I’m simply pointing out a safety risk.
It’s not just one article. I’ve personally just seen enough to be extremely wary, including multiple family members who were prescribed contraindicated meds, given completely incorrect advice, inappropriate testing ordered, etc.
Even the NPs know about the online-only 100% acceptance rate diploma mills that are allowed to see patients as independent practitioners with no physician supervision in most states:
As for your cited study, it’s pointing to something very different than what you’re claiming.
Supervising physicians are the ones who take the hit, and it’s no surprise to me that physicians also tend to see more high-risk patients who are more likely to bring about something. Just because something is on the NPDB database does not mean much. A large number of claims on the NPDB are dropped and do not result in any awards.
If you look at the paper you cited it says “Diagnosis-related malpractice allegations varied by provider type, with physicians having significantly fewer reports (31.9%) than PAs (52.8%) or NPs (40.6%) over the observation period.” and that’s with the more complex patients.
I think the key positive for canagliflozin is that it was the molecule that was tested in the ITP and had the positive lifespan results. Empagliflozin (and other SGLT2 inhibitors) are expected to perform similarly by most people, but there is a chance that it won’t or doesn’t. Its similar to Rapamycin vs. Everolimus. All the lifespan tests have been done on rapamycin, but everolimus is very similar to rapamycin, seems to function very similarly, and is likely to have the same lifespan effect. But… there is a small chance that it doesn’t have exactly the lifespan improvement effect or level of impact.
I tried canagliflozin but had what seems to be a relatively rare side effect of extreme exhaustion, so after 3 months I changed over to empagliflozin. Same benefits without that side effect (for me). More details here: Canagliflozin for Anti-aging - One Month and 4 Month Updates
Fournier’s gangrene is deadly - literature cites ~20-80% mortality. The survivors aren’t doing too great either - serious surgery or amputations are common.
A third or so is due to an immunocompromised state (excluding diabetes). Many men. Especially older.
The impact is large enough to be concerned about when you run the risk factors. It’s not just FG, there are risky associations i.e. urosepsis and hypoglycemia (leading to coma or death). If it was just minor side effects - it’s possible to bounce back. Can’t bounce back if death occurs.
About 2 in 10000 young men have neutropenia. Yet why have antibiotics on hand if the absolute risk is so low for the population? The individual =/= population.
When I was taking 2g of metformin daily, I experienced hypoglycemia. I found out when I thought I was having a heart attack and went into the hospital and we found out it was from the metformin. Reduced to 1g a day and symptoms got better. Went to 500 mg a day and even better. Now I cycle 500 mg every other day with no symptoms.
“Just because something is on the NPDB database does not mean much.”
Exactly! Who needs to worry about data when you’ve got countless anecdotes and scare tactics?
If you read your own cited study - they do mention that as a limitation of the study.
“If you look at the paper you cited it says “Diagnosis-related malpractice allegations varied by provider type, with physicians having significantly fewer reports (31.9%) than PAs (52.8%) or NPs (40.6%) over the observation period.” and that’s with the more complex patients.”
From my reading of the abstract, it appears the physicians had roughly 10 times the rate of malpractice claims than the PAs (for instance). So if for 10,000 PAs you have 10 malpractice claims and 50% of those are for diagnosis, that’s 5 misdiagnosis claims per 10,000 PAs. For 10,000 physicians you have 50 malpractice claims but “only” 30% of those are for diagnosis, that’s still 15 per 10k vs 5 per 10k = 3x the rate of diagnosis malpractice claims. I don’t see any data showing that physicians see more complex patients or that this is a factor.