As you know blood glucose levels increase in the elderly, I am 81 and chose to use
empagliflozin instead of increasing my dose of metformin. This is from a source referenced by the source you provided. It looks to me that empagliflozin is pretty safe. Every drug and supplement from aspirin to rapamycin has risks. One always has to weigh the risk/benefit to decide whether or not to take a certain supplement. If you are young and healthy you probably don’t need any supplements other than rapamycin if you are seeking life extension.
I really like the table.
The bold words are my emphasis.
"Conclusion
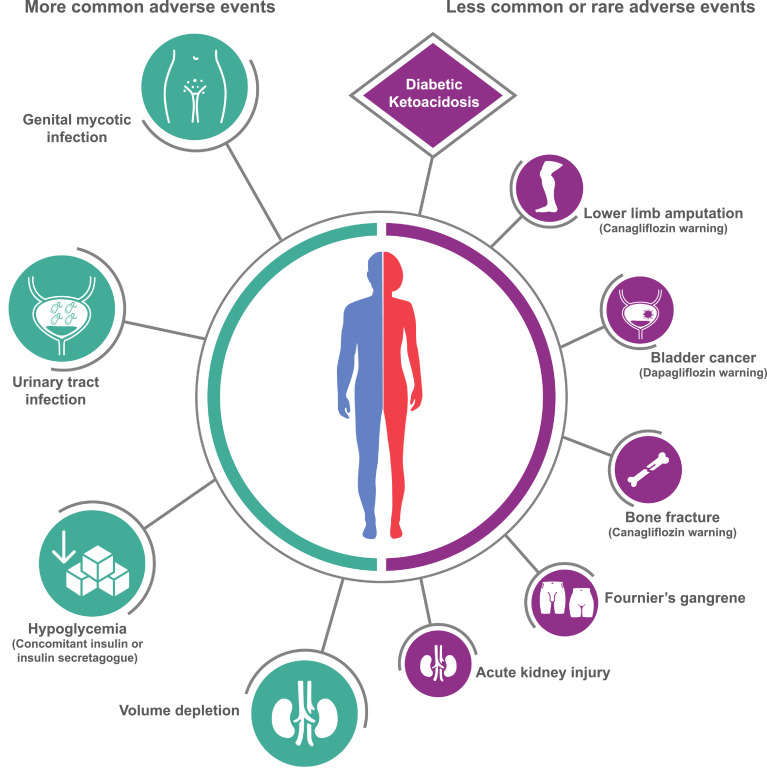
There are strong overall associations of SGLT2 inhibition with protection against major cardiovascular events, heart failure, serious decline in kidney function and all-cause death. SGLT2 inhibitors were also associated
with infections, volume depletion effects and amputation. Some associations appear to differ between compounds."
"Overall, use of SGLT2 inhibition was associated with favourable effects on major cardiovascular events, non-fatal myocardial infarction, hospitalisation for heart failure and all-cause death (Fig. 2). The I
2 statistic indicated a
high likelihood of differences between compounds beyond chance for cardiovascular death (I
2 = 80%) and a corresponding moderate likelihood of differences beyond chance for all-cause death (I
2 = 55%). There was no association of
SGLT2 inhibition detected for hospitalisation for unstable angina or stroke but for the latter there was a moderate likelihood of differences between compounds beyond chance (I
2 = 61%)."
"Effects of SGLT2 inhibitors on kidney disease outcomes
There were just two compounds with data describing effects on the renal outcomes of interest [10,47] and there were strong associations of SGLT2 inhibition with protection against progression of albuminuria and the renal composite outcome"
“Evidence of differences in protective effects was strongest for the outcome cardiovascular death, where empagliflozin appeared to provide a greater magnitude of protection. There was a corresponding, though less strong, finding for all-cause death that was probably driven by the effect on cardiovascular death”
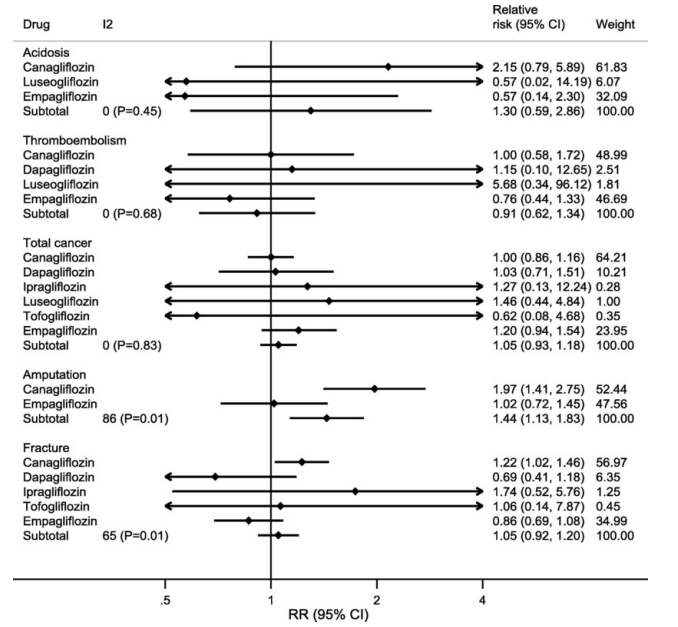
"The association between amputation and use of SGLT2 inhibitors is a new finding that appeared to be restricted to canagliflozin.
“https://spiral.imperial.ac.uk/bitstream/10044/1/66221/2/Effects%20of%20sodium-glucose%20cotransporter%202%20inhibitors%20on%20cardiovascular%20disease%2C%20death%20and%20safety%20outcomes%20in%20type%202%20diabetes.pdf”