A few papers looked at mortality rates and compared the various SGLT2 inhibitors (although, bear in mind that SGLT2 inhibitors only arrived in the market in 2012, so it’s fairly recent to conclude):
Canagliflozin, dapagliflozin and empagliflozin all had a beneficial effect on all-cause mortality compared with placebo. In head-to-head comparisons, the analysis suggests that empagliflozin is superior to both canagliflozin and dapagliflozin. No other head-to-head comparison of any pair of treatments (including non-SGLT2 treatments) found a significant difference between agents, though for most of these comparisons, the 95% CI was wide.
The HRs for all-cause mortality in empagliflozin (N = 16 738), dapagliflozin (N = 26 208), canagliflozin (N = 14 543), and sotagliflozin (N = 11 806) were 0.86 (0.69-1.08), 0.83 (0.72-0.97), 0.86 (0.75-0.97), and 0.95 (0.81-1.11), respectively. […] Canagliflozin possibly reduces both all-cause mortality and CV mortality, whereas dapagliflozin may reduce all-cause mortality but not CV mortality. Empagliflozin and sotagliflozin may reduce neither.
Canagliflozin is especially associated with an increased risk of lower-limb amputation than empagliflozin. Dapagliflozin has a high risk for toe amputation. […]
The risk for diabetic ketoacidosis is highest for canagliflozin, followed by empagliflozin and dapagliflozin. […]
Ertugliflozin and canagliflozin have been associated with euglycemic DKA. However, other SGLT-2 inhibitors also have a risk for euglycemic DKA. […]
A recent pharmacovigilance study conducted FDA’s Adverse Event Reporting System (FAERS) database revealed that canagliflozin had a significant association among SGLT2 inhibitors for acute kidney injury. […]
Statistical analysis of 22 RCTs indicates that dapagliflozin is associated with bladder cancer. The use of dapagliflozin is not advised in patients with active bladder cancer. However, the meta-analysis revealed that SGLT2 inhibitors were not significantly associated with an elevated cancer risk compared with comparators. […]
Canfliglozin is associated with an increased risk of hyperkalemia, especially when combined with ACE inhibitors or ARBs in patients with renal impairment.
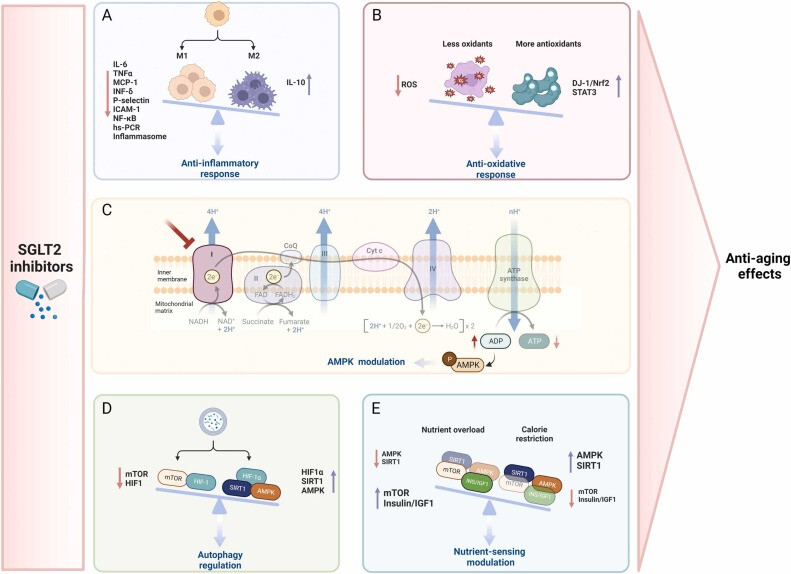
“However, in patients without T2D, these drugs induce small to negligent A1c reductions because the urinary glucose losses are offset by augmented hepatic gluconeogenesis.11,12 In normotensive, nonobese individuals, SGLTi-induced changes in BP and weight are minimal to absent.12 Yet, in all patients, the SGLTi-induced glucosuria and natriuresis bestow cardioprotective and renoprotective actions such as decreasing preload and afterload in the heart and suppressing sympathetic overactivity.9” https://www.sciencedirect.com/science/article/pii/S0033062023001068?via%3Dihub#bb0045
You definitely drop weight, BP, and HbA1c on CR. Weight and HbA1c aren’t affected so much by fasting because most people don’t fast long enough (especially if you mean TRF rather than actual fasting).
As @RapamycinCurious noted above “in patients without T2D, these drugs induce small to negligent A1c reductions because the urinary glucose losses are offset by augmented hepatic gluconeogenesis”
Neither fasting nor a low-carb diet extends lifespan, absent calorie restriction. And I don’t know of any reason to think that low-carb diets would have SGLT2i’s observed effects on heart failure, CVD, or renal disease absent calorie restriction.
By the way, someone mentioned the risk of hypoglycemia with SGLT2 inhibitors. According to this 2023 review among diabetic and non-diabetic CKD patients, it is low (but worth exploring more…): “Data from early clinical trials of SGLT2is have shown that these drugs reduce glycated hemoglobin levels by 0.5–1.0% without causing hypoglycemic events [9]. This occurs because the glucose reabsorption threshold at the tubular level is reduced by these drugs to values not lower than 75 mg/dL, well above the threshold for symptomatic hypoglycemia [10].” (SGLT2 Inhibitors in Diabetic and Non-Diabetic Chronic Kidney Disease)
I’m also struggling to find good data for glycated hemoglobin (HbA1c) reduction among non-diabetic people. This small trial (n=40) found that 6 months of dapagliflozin led to a decrease in HbA1C from 5.8 ± 0.4 to 5.6 ± 0.2. However, this is not even statistically significant (p-value of 0.404, see Table 3). Even acarbose reduces HbA1C more significantly: “A Cochrane meta-analysis found that acarbose therapy reduced glycated haemoglobin (HbA1c) levels by a mean of 0.8%. This decrease was accentuated in individuals with higher baseline HbA1C levels (baseline HbA1c of <7%, 7–9%, and >9% had decreases of 0.56% (95% CI 0.36 to 0.76), 0.78% (95% CI 0.63 to 0.93) and 0.93% (95% CI 0.53 to 1.33), respectively).”Review: Acarbose: safe and effective for lowering postprandial hyperglycaemia and improving cardiovascular outcomes - PMC
This one from 2022 is way larger, with about 3,000 non diabetic patients: Empagliflozin for Heart Failure With Preserved Left Ventricular Ejection Fraction With and Without Diabetes. It reached the same conclusion: “Empagliflozin reduced HbA1c levels only in patients with diabetes and only moderately, with a mean difference in change as compared with placebo of −0.19% at week 52. This latter result likely reflects good glycemic control in the diabetes population at baseline with an HbA1c of 7.3%. Hypoglycemic episodes occurred more frequently in patients with diabetes, whereas diabetic ketoacidosis occurred only in these patients, without differences in the 2 treatment arms.”
All good digs. You bolded the first two phrases in that sentence, but I’ll draw attention to the last one: “without differences in the 2 treatment arms.” IOW, there was no more hypoglycemia or ketoacidosis in the emppagliflozin arm than in placebo, even amongst diabetic patients.
This is my experience. SGLT2 did not lower my HbA1c. I am not diabetic but have been pre-diabetic. I am switching from Farxinga to Cana to see if I get a different result.
So far, none. I have significant reactive (postprandial) hypoglycemia, diagnosed after a 6-hour oral glucose tolerance test (OGTT)… I tried acarbose to treat my reactive hypo, and it helps a lot, but:
It decreases Hb A1c, and mine is already low,
Acarbose only prevents the degradation of complex carbohydrates, so it doesn’t work for simple carbs, and I still have reactive hypo when I eat those,
The amount of complex carbs in the meal determines the effectiveness of acarbose, so I feel like I need to guess and adjust how much acarbose I take before each meal, depending on the expected carb content (and at friends or at the restaurant you never know ).
I’m also interested in SGLT2i because I like drug repurposing. I think there are many low-hanging fruits among existing drugs that are not exploited because of a lack of commercial incentives. The EU wants to create a new incentive scheme for repurposed drugs. If big enough (so far, their proposal is too weak IMHO), these incentives could trigger a new industry: you identify promising candidates for repurposing (let’s say, “empagliflozin for Parkinson’s”, “semaglutide for Alzheimer’s”, etc.), run a cheap trial (you can often skip phase 1 for repurposed drug and then combine 2 & 3), get approved, and cash in the gov money/incentives. Here’s our policy note on the topic: EU Pharma Directive & Regulation Drug repurposing incentives - Google Docs (Feedback welcome!)
I love your group’s efforts at encouraging drug repurposing… definitely a huge opportunity to help people. The balance is always to incentivize the Pharma/biotech groups to do the trials on the new indication, but balance that with the need to keep prices as low as possible. Have you and your group reviewed the A4LI proposals in this area? The Advanced Approval Pathway for Longevity Medicines - a4li.org
In an ideal world, you could say that repurposed drugs (or any drug or intervention, including nonpharmaceutical ones actually) get x% of how much they help the healthcare system save over the next n years. It could take the form of an advance market commitment between the payer (private or public healthcare insurers) and the pharma company before the trial starts.
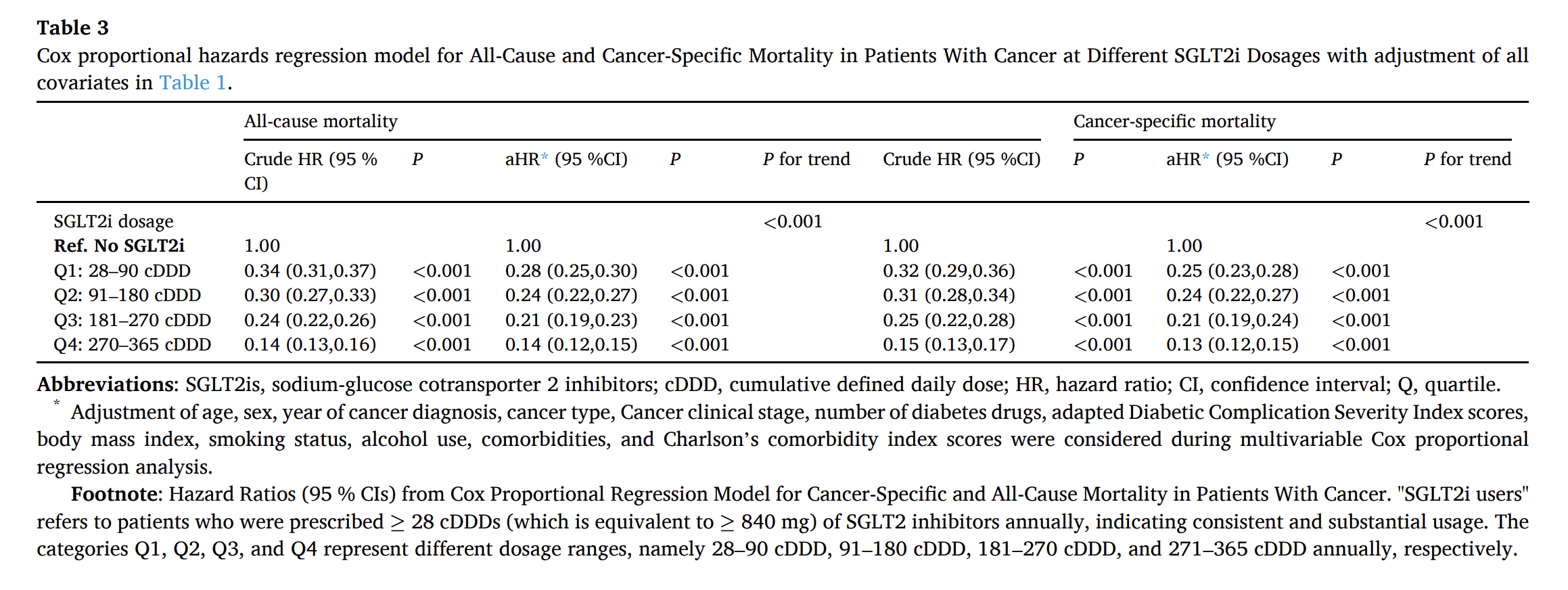
Taiwanese researchers found that SGLT2 use divided death by about 5 in cancer patients (adjusted hazard ratio (aHR) for all-cause mortality in SGLT2i users compared with nonusers of 0.22 (95 % CI: 0.21–0.23)) and that “mortality was noted to significantly decrease with increases in dosage”.
Crazy… (365 cDDD = daily use over a year, with the defined dose defined by the WHO, so for instance 10 mg/d for dapagliflozin or 17.5 mg/d for empagliflozin: WHOCC - ATC/DDD Index )
Thanks. Thats a gigantic effect. I couldn’t find info about variation between SLGT2 drugs. Would the SLGT2 and SLGT1 inhibitors (Cana) have a greater effect than SLGT2 only (dapa, empa)? I wonder.
Yes, it’s almost too good to be true. Even a few months of use (cDDD < 90) have a massive impact. There may be biases in the study, or maybe SGLT2 inhibitors are more potent in the Taiwanese population? In any case, we need more studies to confirm these protective (or even curative?) effects. AstraZeneca is running a massive cohort retrospective study about this with more than 1 million people, results expected in 2025: Cancer in Patients on Dapagliflozin and Other Antidiabetic Treatment
There are other ongoing trials on SGLT2i + cancer:
“Canagliflozin, the other dual SGLT inhibitor, is more selective to SGLT2 than SGLT1 compared with sotagliflozin (250-fold vs 20-fold, respectively). “
It looks like Cana does have a smaller (order of magnitude less) effect on sglt1 than sotagliflozen. I don’t think the other popular SGLT2 inhibitors have any sglt1 inhibition. Is the the sglt1 effect important to the longevity benefits? I wonder…
However, according to SGLT inhibitors for improving Healthspan and lifespan: “Empagliflozin, dapagliflozin, and sotagliflozin are the agents in the SGLTi drug class with the strongest safety and efficacy for improving healthspan and lifespan.”