Yes, this is supposedly a big problem in “real world” using SLGT2i in men. This concern was raised by a colleague of mine, she is a professor of clinical diet and functional medicine (MD) and raised that as a major risk. She also pointed that in active people they can lead to RED-S and that risk of euglycaemic ketoacidosis , serious complication, is often overlooked.
2 Likes
But since the overwhelming majority (99.9999+ %?) of SGLT2i drugs are used by diabetics, who are all immunosuppressed to a greater or lesser extent, I’d expect infection risk to be much lower in a non-diabetic user with a healthy immune system, wouldn’t you?
5 Likes
The infection risk is much lower in non-diabetics. I take a cranberry supplement preventatively.
3 Likes
Lately is also prescribed (at least in EU) for CV prevention to pre diabetics (HbA1c above 5.7).
All three conditions I mentioned are easily overlooked as yeast UTI is mostly asymptomatic in case of absence of complications. RED-S and euglycaemic ketoacidosis have really non specific symptoms and are mostly overlooked. Euglycaemic ketoacidosis is a more specific diabetes condition and probably risk in non diabetic is negligible but still present I guess.
My Methylene Blue arrives this weekend. My IQ will be 25 points higher by Monday! Or I’ll just have blue teeth.
7 Likes
Besides depression (and the two may actually be linked), longitudinal studies seem to hint at a powerful neuroprotective effect of SGLT2 inhibitors: Meta-analysis of Association between Newer Glucose-Lowering Drugs and Risk of Parkinson’s Disease (Sept 2023)
SGLT2 inhibitors were significantly associated with a lower Parkinson’s disease risk (OR: 0.37; 95% CI: 0.13–1.01) than placebo. The neuroprotective effect is not only due to glycemic control, as other anti-diabetic drugs do not perform as well.
4 Likes
I can confirm that you will NOT be 1 point higher on your IQ and will definitely have blue teeth lol.
Did 20 drops a day for about couple weeks while back, couldn’t say anything bad or good. I might have felt a bit stronger (e.i. felt a bit easier than usual carrying 40 water bottles from Costco) but then could have been other things I do. as far as alertness or sharpness didn’t feel that at all.
5 Likes
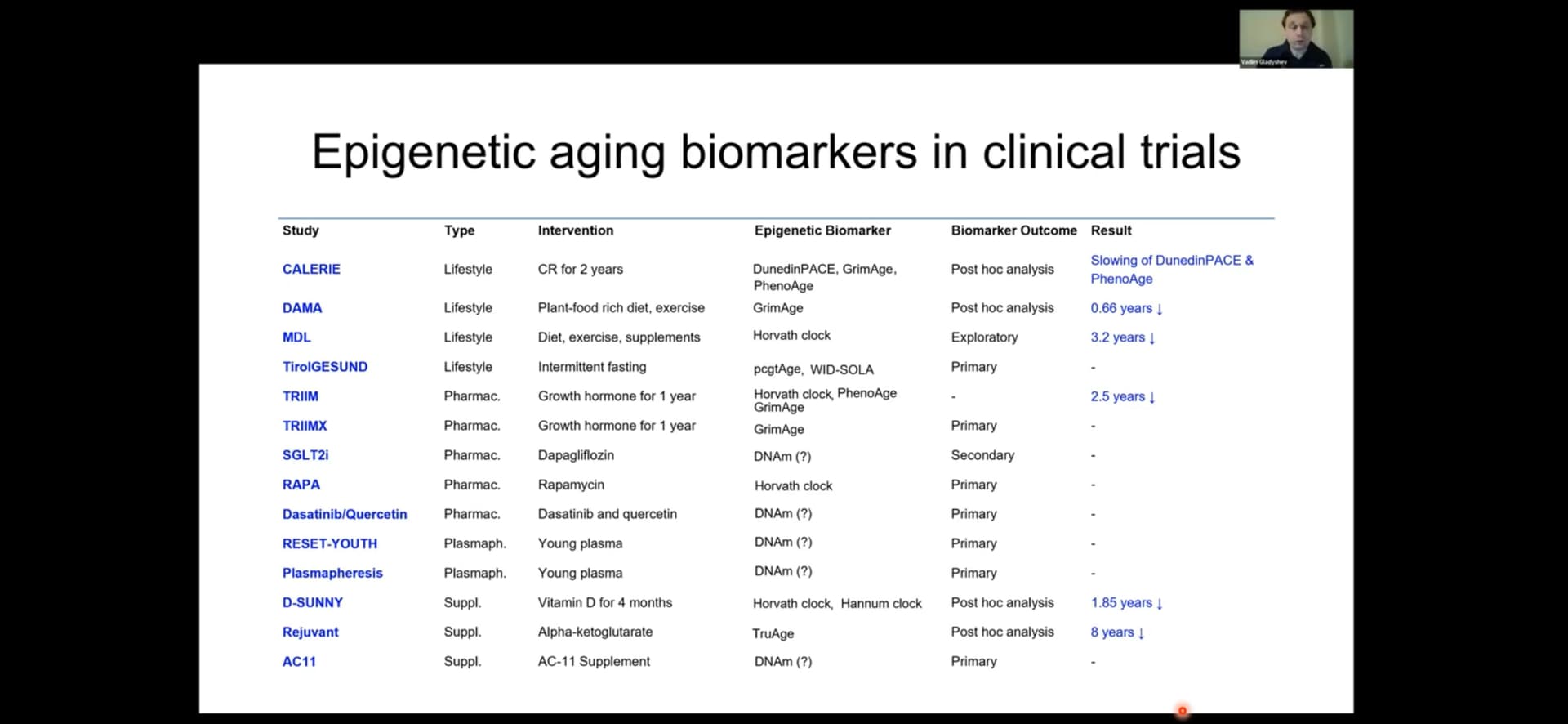
Anyone have any sense of what this SGLT2i and/or rapa trial is?
In Dr. Attias new video Dr. Miller said the most recent ITP Canagliflozin trial increased male life expectancy but DECREASED female mouse life expectancy. He believes this to be a dosing issue. Higher doses may decrease life expectancy. Even though both males and females received the same dose he believes that the liver enzymes difference between males and females ended up giving the females an effective higher dose.
Low doses may be more beneficial than high doses.
7 Likes
Thanks @DeStrider . Please note that I am talking about a clinical trial - aka in humans.
(Different from a rodent study).
I had not previously seen any direct aging measurements of Cana / SGLT2i, or according to the Harvard prof at least Epigenetic data from humans, so interesting in what the trial he referred to is.
In the prof’s same list (see above, and reproduced below) he also says there is a clinical trial / human trial of rapa with epigentic age measurements.
Do not think this forum or Dr Attia has commented on either of those and seems like extremely valuable info.
All of these are clinical / human - and all have some epigentic age measurement component.
2 Likes
From this talk (people may enjoy for other reasons too):
2 Likes
The problem is that epigenetic age measurements are not accurate. As Dr. Miller said, when you are sick, your epigenetic age increases. When you get better it decreases. When a woman is pregnant, her epigenetic age increases. When she gives birth it decreases. When you have a deadline at work, your epigenetic age increases. When it’s past your age decreases. I’m not sure how much trust I can put in epigenetic tests.
2 Likes
I’d still take nice info + human epigentic age info vs only nice info
Or you saying you’d prefer to not look at human epigentic profiles of someone taking rapa or Cana/SGLT2i?
Many of the effects you mentioned in your last post should be controlled for/aberage out with group sciences in a clinical trial
There are enough ultra smart and credible profs feeling that there is value in epigentic profiles that I’d rather look at that info than not (Levine, Horvarth, Gladyshev) even if one should look at it with caution.
I agree it’s the early days of epigentic clocks
But even Rich Miller - on last week’s Peter Attia podcast - proactively mentioned work on epigentic clock stuff in the context of ITP’s post experiment tissues - so your read seems perhaps more negative than his own current/latest read
You can put as much faith as you’d like in epigenetic tests. However, to me, they’re not developed enough to provide much useful information for the cost. I’ve taken many of these tests and they’re all over the board for me. Anywhere from 20 years younger to 20 years older. That’s a pretty wide range.
It’s like if I were to ask you to guess how many marbles are in a jar and you told me somewhere between 5 and 20,000.
Also, my father and I both took epigenetic age tests and we both came in at 12 years older. I take Rapamycin and he doesn’t. He goes to the gym 3X a week, is a vegetarian, and weighs 150 lbs. I don’t go to the gym, am an omnivore, and weigh much more. If the healthiest guy I know has an age 12 years higher than his real age 89 vs 77, I really have a hard time trusting epigenetic tests.
Aging.ai said I was 20 years younger and Levine said I was 10 years younger. After taking Rapamycin, my epigenetic age decreased 7 years, my aging.ai age went up 10 years and my Levine age stayed the same. What should I make of that?
2 Likes
Not sure if we somehow have diverged to having different conversations.
I was never arguing that they are ready to be used as a predictive measure at the level of a given individual
But would still prefer to see the data from those measures from longevity clinical trials in humans than only rely on mouse data.
The human epigenetic data will have issues. But so does the mouse data when making human decisions.
1 Like
Yes, the more data the better and human data is better than mouse data.
2 Likes
I agree. Rationally I can’t say out loud that more information isn’t better. But I do think about how much bad or misleading information I should let get into my head for my emotions to work on.
For example, an MRI of an older persons knee would not look like a 20 yo knee. It would (probably) look like something is wrong. But most likely nothing is “wrong” based on what can be seen. Even if there is pain, the structures seen in the image were probably there before the pain started. So how much help did the MRI information add to my decision making ability?
I am not getting an epigenetic age test yet. I will get one when the tests mean more than they do now. It’s a personal choice for sure.
3 Likes
Totally hear you. And think they make more sense in group settings so far as a clinical trial when you can compare the intervention vs control across many and look at the averages.
Still having said that, I think I’ll personally build up some individual epigentic tests on myself also so that I can have the time series to look back on in the future
- it’s also seems like later algorithms might be possible to run on todays data, think some of the companies are even offering to do that as the clocks and algo’s get better in the future “backward compatibility”
2 Likes
Looks like dapa is safer indeed: Sodium-Glucose Transport Protein 2 (SGLT2) Inhibitors - StatPearls - NCBI Bookshelf
Also, dapagliflozin is the only one available in generic as of today in Canada and the EU. (In the US it’ll be available in Oct 2025)
3 Likes
And, it is available from all of the usual Indian suppliers.
2 Likes