CTStan, here is a link to the document.
I use this one.
Manual calibration for BP and I check it once a month and it appears to remain reasonably accurate.
Takes BP every 5 minutes.
2 Likes
Very reasonable cost.
FWIW
I looked at the “CardiacSense” watch, list price in the UK*, cost is over 825.00 GBP. I do not think may consumers will purchase at 825.00 GBP
- The UK distributer site posted a price, others distributer did not post a price.
The other reason I bought the Aupalla was that from what I could see, it was the only providing HRV data without having to take out a monthly subscription.
2 Likes
@tongMD - I love this whole approach!
Create a model (of the current understanding) based on the systems and pathways that effect aging recognizing the genetic differnces that can alter the process.
You just summerized about 100 years of what we understand about aging and showed by adding software advances, that hopefully accelerate our prediction process that is light years ahead of what we have been doing. One of our biggest problems in medicine is everything is slow! Slow to share data, slow to come to conclusions without decades of RCT and slow to address integrate most of what you just typed out in 4 paragraphs.
Let me know when you create an app to input data that can generate some reasonable options beyond what most of us have to do…and just guess!
2 Likes
Welcome to the forum and thanks for the detailed overview of your regimen, supplements, medications.
I love the in-depth analysis for potential drug/drug interactions, etc. Ideally it would be something we all could do.
I just wanted to pull out links to all the sited and resources you referenced:
NIH-Library of Integrated Network-Based Cellular Signatures
https://lincsproject.org
Universal Natural Product Database
https://bioinf-applied.charite.de/supernatural_new/index.php
Kyoto Encyclopedia of Genes and Genomics
On a related issue, I’ll see if I can get Matt Kaeberlein and Mitchell Lee to share the outcomes of outcomes of testing of the combinations of the more common supplements and rapamycin, SGLT2 inhibitors, Acarbose, etc. that people here are using - to see if the combinations are synergistic or counterproductive. This type of information is probably something they’ll get as part of their research, and would likely have little or no commercial value by itself - so I’m hoping they will be predisposed towards releasing this basic information for us.
See: Ora Biomedical: Matt Kaeberlein's New Longevity Biotech Company
5 Likes
From my understanding, Dr. K didn’t want to test acarbose in dogs because it would decrease compliance due to GI toxicities, rather than worrying about potential drug-drug interactions of acarbose with rapamycin. I suspect he currently believes it would be close to additive but I’m not sure.
As for his newest startup - it’s an interesting concept and I look forward to it - there will be a lot of great outcomes from novel or optimized methods involving high throughput screening as a field. I’m more focused on what I can apply directly as of now or in the near future with the best odds, information, and models available.
The main risk I worry about for my situation with acarbose is possible hypoglycemia (primarily mitigated by an accurate enough CGM with a hypoglycemia alarm) with any herbs or foods that affect AMPK activation directly or indirectly, on top of intermittent fasting and intense exercise. So far, no hypoglycemia.
I will also note I’m going on a bit of a departure from the literature with acarbose (partly from a few suspicions that it won’t necessarily pan out in real-world humans), so it could end up being no additional effects if the effect is not because of postprandial glucose levels. I’m not taking acarbose all the time and I’m not taking it with rapamycin together - just high carb meals prn (if I’m at a restaurant due to social reasons and end up eating a high carb meal very occasionally a few times a month) and I take only 25 mg acarbose separate from other compounds (about 12-20 hrs apart) beyond any potential dietary nutraceuticals. Very little is absorbed systemically and all of that is excreted quickly in urine. Most acarbose is eliminated in the feces. The remaining metabolites take a bit longer, but I think at the 12 hr mark it’s probably insignificant if those metabolites (or any related effects from acarbose) even have activity. I’d probably be more concerned about any potential acarbose drug interactions that are significant if it’s closer to the first few hours after ingestion.
I would note there are dietary sources of alpha-glucosidase inhibitors that I take. An obvious one is an anthocyanin from steamed sweet potatoes (traditional Okinawan diet staple) that is stabilized after steaming to inactivate peroxidase.
My pure speculative guess is multiple natural alpha-glucosidase inhibitors taken in food form already indirectly naturally tested in a population that appear to have a high average life expectancy partly based on mild calorie restriction (mTOR inhibition, but acts differently) and indirect intermittent fasting (via light evening meal or skipping dinner) is the better choice. I suspect using only acarbose as the single alpha-glucosidase inhibitor will run into problems when it comes to real-world translational results.
Not to mention, there’s a suggestive additive effect with rapamycin - it appears to be very low-hanging fruit so far when tested in mammals.
2 Likes
I would like your thoughts on time-restricted feeding
As a child, I never wanted to eat breakfast and couldn’t figure out why everyone was force-feeding me. As I grew up I adopted the social norm of having breakfast. After I retired I needed to lose some weight, so along with exercise, I did a keto diet until I reached my own goal of 175 lbs. Then I just did time-restricted feeding. I do ~ 18/6, not because I have a strong belief that it is optimal, I just don’t feel hungry before 1 PM. My first meal is at noon because that is convenient for me. The plan is working so far and I eat a somewhat South Beach Diet, again by natural choice and not by plan. I do not count calories and I eat until I am full.
So, do you think I should force myself to eat earlier in the day as some proponents of time-restricted feeding advocate?
3 Likes
I don’t eat too late (last meal >3 hrs before bed) because there is suggestive evidence of “fasting while sleeping” on glymphatic processes that may offset or delay dementia (fun fact - Alzheimer’s used to be my white whale).
It also consistently affects my sleep (actigraphy & subjective feelings), so I almost never do that anyways.
I’m shooting in the dark with timing and IF in the first place - it’s weak evidence in human trials compared to say traditional Mediterranean diet (see Cochrane review) and it’s speculative. I first got the general idea from traditional Okinawans eating more earlier in the day and little towards the end (or skipping dinner) - before IF went sort of more mainstream and they seem to have better sleep. My IF 16/8 probably does not result in significant weight loss, all else equal.
I’m assuming getting to a fasted sleep state quicker is generally better. It takes ~6 hrs to digest your food but there are ways to transition slightly quicker that I do personally - i.e. light dog walks after last meal, less fat in last meal. (I don’t do intense exercise right after eating or taking things like metformin - it’s too sharp of a transition)
I occasionally shift a bit to 11am-7pm in terms of occasional (~2-3x a month) social functions where eating is involved, but otherwise consistent timing.
One of the reasons why I refrain from taking things like metformin, berberine, and/or acarbose all the time is I worry about hypoglycemic responses which can depend a lot on individuals and I don’t like relying on subjective feelings based on my experience of talking with diabetic patients who ended up with a CGM.
Review of the proposed mechanisms (I suggest reading it entirely and going through all the references):
3 Likes
Thank you for taking the time to share your experience.
Both the keto diet and time-restricted feeding raise my morning blood glucose levels while lowering my HEMOGLOBIN A1c levels.
Do you think perhaps A1c level may be a better marker than fasting glucose level for those on keto or time-restricted eating protocols?
I personally use a CGM with relatively high accuracy as my primary data source for glucose changes and computation of autocorrelation functions (there are some issues, but minimized). I do take HbA1c regularly for reference and fasting glucose comes with the lab bundle.
In diabetes screening, HbA1c and fpg are both used. Fpg is not great because stress can easily throw that out of whack, so I wouldn’t rely on that over 2 hr oral glucose test.
There are pitfalls with HbA1c in various clinical scenarios (ie in my case, when I donate blood it is falsely lowered) but it’s a better index of averaged glycemic exposure since RBC live for ~120d.
2 Likes
@desertshores - Charles, this is simplistic, but Dr. Fung does a good job in breaking down the studies of fasting and time restricted eating. He has benefited from the popularized fad component, but I still think has some basic values that apply. Also, Dr Longo out of USC longevity center, does a nice job of breaking down many of the studies on fasting and time restricted eating with most interesting being benefits of cancer prevention and fasting before chemo treatments to enhance normal cell protection from chemo and higher sensitivity of cancer cells to chemo. He is the inventor of the Prolon diet or fasting mimicking diet that promotes benefits of fasting without the loss in muscle mass.
 | Jason Fung")

1 Like
I think this belongs here:
I like Dr. Attia’s approach. I still think Dr. Tong @tongMD is ahead of the curve with his software algorithm approach.
I start with risk of do nothing vs. risk of therapeutic option. Next step, is there a subjective change to warrant the risk of taking the therapy? - For example in hormone replacement, is there an improvement or resolution of hot flashes, night sweats, libido and mood. If there is not, then probably not worth any risk, if there is then weigh it out for the individual. Is there objective metrics that has data to support the a change a lab or measurement that is supportive of continuing treatment. Example might be a change in vitamin D level, improvement in A!c level or even cholesterol that support the use of the therapy even if no subjective improvement. Lastly, even though no subjective or objective changes or measurements, the risk vs. benefit for the individual is worth taking the therapy - a 20+ year old taking Rapamycin despite no subjective or objective improvements.
Thanks for sharing this!
3 Likes
Related to this Attia referenced post, some thoughts:
-
Matt (MK) responds, “I think it depends on the biomarker you’re talking about.”
-
If you’re talking about a biomarker of efficacy for aging, he agrees that we don’t have that for anything because we don’t have any biomarkers of efficacy for aging (MAC: aging clocks? but hotly debated. We have ever deeper and more powerful GWAS of longevity cohorts teasing out longevity genes/pathways, how to translate to a biomarker?)
-
But we do have clear biochemical biomarkers, certainly for rapamycin (MAC: true)
-
We know rapamycin is a very specific inhibitor of mTOR, and we have good biochemical ways to measure mTOR inhibition (MAC: yes in mice after we kill them, humans not so)
-
The challenge is we don’t know what level of mTOR inhibition is optimal for aging, and that gets back to the aging biomarkers (MAC: not true, we know VERY WELL in mice the level of mTOR in various tissues associated with aging, thoroughly documented after we euthanize them. We don’t know the human translation; so he likely was talking about humans)
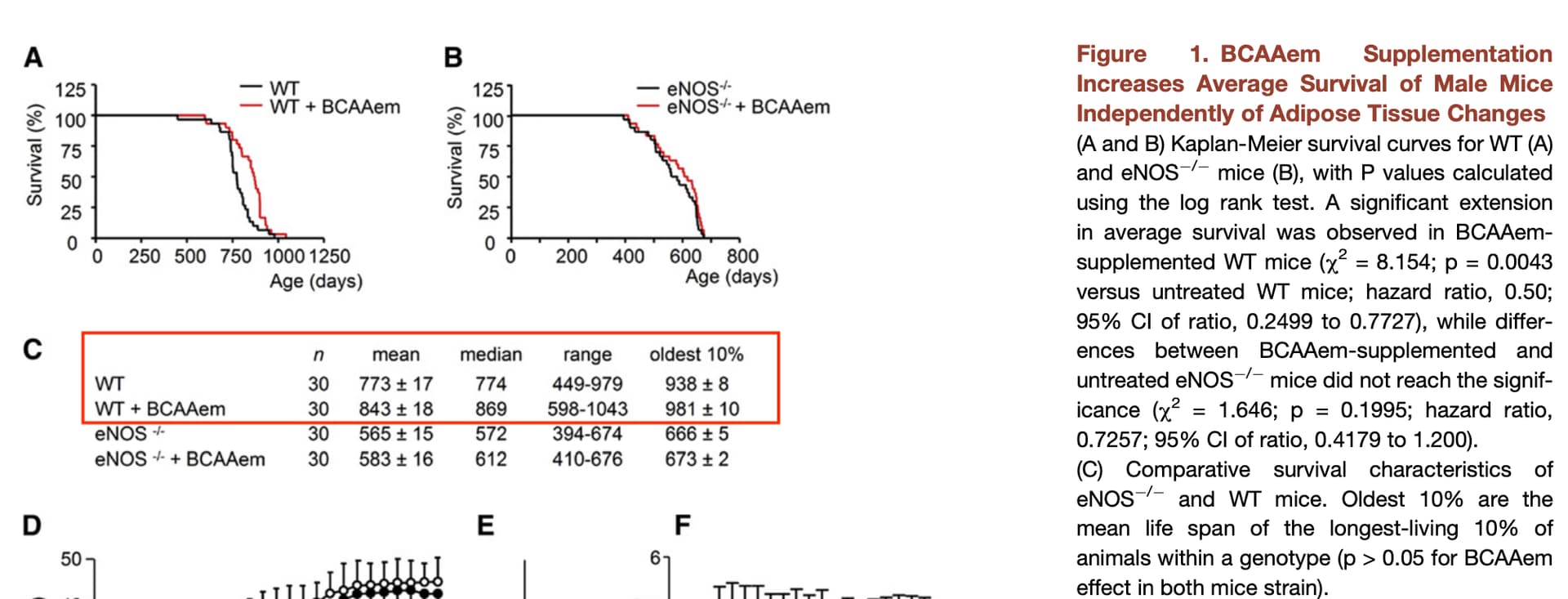
I’ll add in this study, that BCAAs which are well known for mTOR activation, yielded an average longer lifespan in middle-aged mice (sort of the opposite of what one would expect if it was only about mTOR inhibition), partly from SIRT1
https://www.cell.com/cell-metabolism/fulltext/S1550-4131(10)00304-9
2 Likes
More average survival (9%) than lifespan (4.5%)…not at all close to rapamycin longevity efficacy in the WT mice (see red box below) mTOR is still king.
So does eating enriched BCAA improve healthspan, but as expected, not increase lifespan…at least, not curtail it? mTOR absolutists would say no, BCAA bad.
Although there are many more studies showing increased BCAA indeed reduces lifespan.
What if they did BCAA supplementation AND Rapamycin together?
Wait did you mention SIRT1…buried for dead? Sinclair is smiling.
1 Like
@MAC @tongMD I really like this discussion!
A healthy 25 y/o has peak levels of IGF-1 and testosterone. Most have do not have signs of age related disease or symptoms of age related high mTOR stimulation.
Now take the same person and move them to 50 y/o. IGF-1 and testosterone levels are lower - mTOR seems to get stuck in constant “overdrive” and by inhibiting it with CR, Metformin and Rapamycin, we see a reversal of signs and symptoms of aging and longevity. However, if you take the same 50 y/o and just replace the testosterone and IGF-1, at least anecdotally in many patient populations, you see a reversal of many symptoms of aging and many claim feeling more youthful.
My point is that there must be much more going on than a simple on and off mTOR signaling. What is the difference from young people mTOR vs. older mTOR and can we use this model to better control aging? Is it just that old cells ( shorter telomeres ) respond differently? Many people on this site do both - stimulate mTOR with exercise, higher protein diets, testosterone replacement, peptides to enhance iGF-1 / GH and at the same time do pulsed Rapa, take Metformin, practice CR and fasting. Is this just a battle of Healthspan vs. Longevity? If we had the experts in the Rapa / mTOR field - that would be the question I think is the most interesting.
5 Likes
Almost all growth factors increase cellular proliferation and lead to a short term youthening effect. We’ve seen this with growth hormone, androgens, and vascular endothelial growth factor. Many times up regulation of telomerase is part of the equation as well.
Over the long haul the effects are pro aging due to hyper function, senescence, telomere shortening, etc.
6 Likes
Sure! All good points. So why does up regulation of mTOR from aging not cause a youthful effect. Why does high levels of growth factors not seem to be as harmful to people when they are younger? A few of the forum members that take TRT, say they understand it may not help with longevity or even shorten it, but feel the QOL is worth it. I like the Telemorase point since it could be the duration of exposure that is what is important - old cells vs. young cells.
Thanks for your points!
3 Likes