
Executive Summary
The primary focus of this analysis is the Morin et al. (2024) study published in Aging Cell, which utilized UK Biobank data from 500,000 individuals to evaluate the association between 406 commonly prescribed drugs and all-cause mortality. The study identifies a profound “survival bias” in pharmaceutical data: 92% of drugs are associated with increased mortality because they are markers for underlying pathology. However, a select group of 14 compounds demonstrated a statistically significant reduction in mortality risk, most notably SGLT2 inhibitors (33.6% reduction) and PDE5 inhibitors (14% reduction).
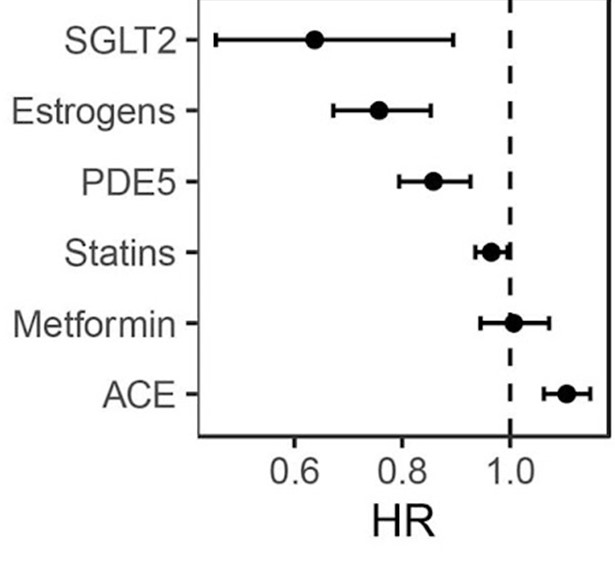
The findings challenge the “Metformin-first” longevity narrative, as Metformin showed zero mortality benefit in non-diabetic cohorts within this dataset. Conversely, SGLT2 inhibitors emerged as the superior class for systemic cardiorenal protection. Estrogen replacement therapies also showed strong protective signals (24–33% reduction), reinforcing the “window of opportunity” hypothesis for hormone replacement therapy (HRT) in post-menopausal health. While the study is observational (Level C), it provides a roadmap for repurposing existing, safe pharmaceuticals to modulate human aging. Crucially, the analysis highlights a massive translational gap for ITP-validated compounds like Rapamycin and 17-alpha estradiol, which lack large-scale human mortality data despite robust success in murine models.
II. Insight Bullets
- SGLT2i Dominance: SGLT2 inhibitors (e.g., Empagliflozin) provide a 33.6% reduction in mortality, significantly outperforming Metformin in systemic risk reduction.
- The Metformin Myth: Observational data suggests Metformin’s benefit is largely restricted to diabetics; it failed to move the needle for all-cause mortality in healthy UK Biobank participants.
- PDE5i Cardioprotection: PDE5 inhibitors (e.g., Sildenafil) are associated with 14% lower mortality, likely due to improved endothelial function and reduced systemic blood pressure.
- Estrogen Efficacy: Estrogen patches (Estraderm) and tablets showed the highest protective association among women, with a 33% and 27% reduction in mortality risk, respectively.
- Disease Confounding: 92% of drugs appear “lethal” in data (e.g., Opioids at +450% risk) because they are proxies for terminal or severe illness, not due to direct toxicity.
- SGLT2i Mechanism: Beyond glucose lowering, SGLT2i’s benefit stems from reduced renal workload and direct cardioprotective signaling (cardiorenal axis).
- 17-alpha Estradiol: This non-feminizing estrogen extends male mouse lifespan by 19% but currently lacks human mortality data.
- Age-Dependent HRT: Benefits of estrogen are most pronounced when initiated in the 50–59 age bracket; later initiation yields diminishing returns.
- Statin Subtlety: Despite massive use, Statins (Atorvastatin) showed only a modest 3–9% reduction in all-cause mortality in this cohort.
- Endothelial Aging: PDE5 inhibitors likely provide “bio-identical” support for aging vasculature, which naturally loses nitric oxide sensitivity after age 60.
- Cost Barriers: SGLT2 inhibitors cost ~$400–$500/month ($40 to $60 from Offshore/Indian pharmacies) compared to Metformin’s $20, creating a socioeconomic barrier to longevity access.
- ITP vs. Biobank: Rapamycin is the “gold standard” in mice (ITP), but was absent from the protective list in this human observational study due to low prescription volume or specific use cases (organ transplant).
- Anti-Inflammatory Signal: Naproxen showed a 10% lower mortality risk, hinting at the role of “inflammaging” management, though long-term NSAID use carries significant GI/renal risks.
- Antibiotic Outlier: Lymecycline (acne treatment) showed a 31% reduction; this is likely a socioeconomic confounding factor (wealthier/healthier patients seeking skin treatments).
- Hyper-Personalization: The data suggests longevity protocols must be sex-specific (e.g., 17-alpha estradiol for males, traditional HRT for females).
III. Adversarial Claims & Evidence Table
| Claim from Video | Speaker’s Evidence | Scientific Reality (Current Data) | Evidence Grade | Verdict |
|---|---|---|---|---|
| SGLT2i reduces mortality by ~33% | Morin et al., 2024 (UK Biobank) | EMPA-REG OUTCOME confirms 32% reduction in all-cause mortality in T2D. | B | Strong Support |
| Metformin has no benefit for non-diabetics | Morin et al., 2024 (UK Biobank) | TAME Trial (Ongoing) is still investigating this; MILES study showed mixed metabolic signals. | C | Plausible |
| Sildenafil reduces mortality by 14% | Morin et al., 2024 (UK Biobank) | Adesuyan et al., 2024 shows 18% reduced risk of Alzheimer’s/Dementia in PDE5i users. | C | Strong Support (Obs) |
| 17-alpha Estradiol extends male lifespan | ITP Mouse Studies | Harrison et al., 2014 confirms 19% male increase. Human safety data is limited to marmoset pilot studies. | D | Translational Gap |
| HRT reduces all-cause mortality | Morin et al., 2024 (UK Biobank) | WHI 2017 Meta-analysis showed neutral effect overall, but beneficial in age 50–59 cohort. | A | Plausible (Age-Specific) |
IV. Actionable Protocol (Prioritized)
1. High Confidence Tier (Level A/B)
-
SGLT2 Inhibitors (Empagliflozin/Dapagliflozin):
- Indications: T2D, Heart Failure (HFrEF/HFpEF), and Chronic Kidney Disease.
- Longevity Protocol: 10mg Daily (Standard Clinical Dose).
-
PDE5 Inhibitors (Tadalafil):
- Indications: ED, BPH, Pulmonary Hypertension.
- Longevity Protocol: 5mg Daily (Low-dose daily regimen for endothelial health).
2. Experimental Tier (Level C/D)
- Metformin (Off-label): 500mg–1000mg Daily. Benefits in healthy individuals are unproven; potential interference with exercise-induced mitochondrial biogenesis.
- 17-alpha Estradiol: Safety Data Absent for humans. Do not attempt.
3. Red Flag Zone
- Combined PDE5i and Nitrates: Lethal Interaction. Risk of catastrophic hypotension.
- Chronic NSAID Use (Naproxen): Despite the 10% mortality reduction in Biobank data, chronic use risks peptic ulcers and renal failure (Level A evidence of harm).
V. Technical Mechanism Breakdown
- SGLT2 Inhibition (Proximal Tubule): By blocking glucose/sodium reabsorption, these drugs lower glycemic load and systemic blood pressure via osmotic diuresis. They shift metabolism toward ketone body production, providing a more efficient fuel for the aging heart.
- PDE5 Inhibition (Vasculature): Inhibits the breakdown of cGMP in smooth muscle cells. This maintains vasodilation and improves blood-brain barrier integrity, potentially explaining the lower incidence of Alzheimer’s found in longitudinal cohorts.
- Estrogen Signaling (ER-alpha/beta): Estrogen maintains endothelial nitric oxide synthase (eNOS) activity and bone mineral density. In males, 17-alpha estradiol appears to work via the **Aryl Hydrocarbon Receptor (AhR)**and insulin signaling without activating classical feminizing ER-alpha pathways.