I doubt the decision making of people in their 20’s in general and what the drivers are of their effort. If it’s pragmatic for their own longevity or coincidentally because of a research gap, status, money, etc. I meant my question was if they really have to worry for their own chance of reaching LEV if they at 20 years old have an average life expectancy of +60-70 years — much longer than the 10-20 year LEV timeline, and thus how much effort they need to spend towards it. If that question makes sense.
1 Like
Just a friendly reminder, per Matt Kaeberlein - before we show max life extension in humans, we should show it in easier animal models, mammals, which would be mice. The greatest max life extension in mice we have shown, has been CR, which was demonstrated already in the 1930’s. Rapamycin, which has been around for decades, is not quite as effective as CR. And… after pulling out those two, the cupboard is empty. Thank you for coming!
So, for over 90 years now, we have not beat that intervention (CR) even in mice. For higher primates, it’s even worse. Now you are talking about humans?! Lord have mercy.
Given this pace of “progress” (more accurately “stagnation”, as progress is equal to zero for almost 100 years), we really could say there’s been no substantive progress since the time of Luigi Cornaro from the 1400-1500, or 500-600 years ago when it comes to max life extension of human lifespan.
I’m 67 currently. I am convinced, that even if I were to live another 50 years (won’t happen, lol), I will not witness human max life extension. Once I’m dead it won’t matter because I won’t be around to say “I told you so”, but whatever, I’ll still say it: I don’t believe there will be any “escape velocity” for the next 100 years. So, nobody alive today will witness such an event. It’s “prediction”, so naturally I can’t prove it, only wait to be proven right or wrong - but I won’t be around that long. If I get another 30 years (lucky!), I will only be able to be tested for that long… so, we’ll see. My bet is stagnation for the foreseeable future.
4 Likes
It may be physiologically true, but I presume all of us care about living longer not that so that we can sleep more, but so that we can spend more time with family, friends, doing things we enjoy etc.
There are some pretty serious ethical issues with that. The whole “right to try” thing was originally pushed by drug companies as a way to try and market their unapproved products, make profit and weaken regulations. Federal “right-to-try” over a year later: Still a failure and still about the money (and weakening the FDA) | Science-Based Medicine
1 Like
Latest issue of New Scientist with Cover Feature “How to Live to 100”.
Some longevity hacks. Also, happens to feature Bryan Johnson!



If you think about your top 25% probability scenarios, where do think each of these might be in 30 and 50 years?
-
AI + robotics/automation ability to accelerate discovery exponentially?
-
Partial reprogramming? (This is basically what every mother does with her and the faster’s old cells when they make a 0 year old baby - it’s not something that we don’t know if it is possible, every specific of animal on the planet does it perfectly all the time)?
-
Gene/cell therapies advance materially?
-
Organ and tissue manufacturing advances to be replace old parts with one’s own, young (and improved) ones?
-
Always-on biomarkers enable rapid, personalized iteration and stacking?
-
Multi-omics + digital twins make aging measurable and munch more predictable/understandable?
-
Nanomedicine + closed-loop implants repair damage in vivo?
-
Regulatory + financing shifts treat aging as an addressable indication (in 30-50 years, not in 5 or 10)?
1 Like
-
Actually I think it will progress greatly in some areas, such as imaging and protein and generally molecule combinatorics. But that by itself will not result in LE.
-
A lot of reprogramming can happen this way, and will. But it will not result in LE, because no combination of XX and XY has resulted in LE so far (in a few 10’s of thousands of years), telling us there are some fundamental limitations inherent in the human genome.
-
Yes. But no LE, although substantial healthspan extension.
-
Yes, but so what - we already subsume that in point 3 above. Healthspan E, but not LE.
-
Sure. HE, no LE.
-
Yes.
-
Yes.
-
Yes.
You guys are veering off into a discussion on LEV… there is a thread on X right now discussing this:
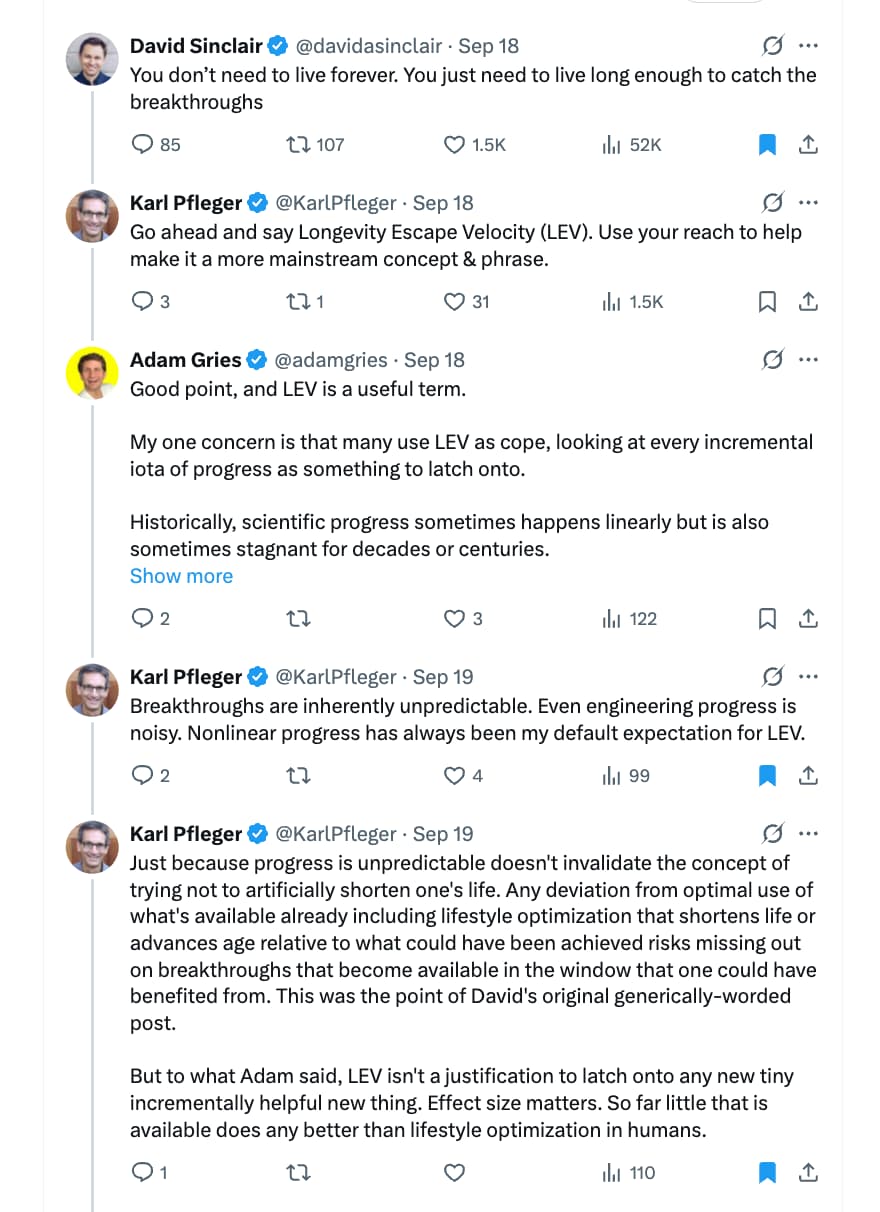


Sources:
I don’t personally think it is that good scientifically as a concept. It is a good clickbaity marketing idea, however.
2 Likes
Basically LEV is a thing, but different people could achieve it at different points and it’s not binary – on a spectrum with different levels of acceleration and deceleration. E.g income like your B-LEV, health, prior LDL-C exposure, suboptimal BP exposure under the curve, kidney function, bone density, etc.
2 Likes
An alternative is to think that there might be a series of bridges ahead of us, and the question is whether we will be healthy enough to reach the next one
and that the value of reaching that bridge has some additional probabilistic value as the beige might help one to reach the next bridge
We can see some of the contours of some key bridges being developed, but we don’t know yet when (or if) a given bridge will be finalized successfully
2 Likes
Yes, why people in their 20s also should care about cancer screening and prevention, perhaps doing an MRI to make sure no aneurism risk, wear helmet when cycling and skiing, etc
2 Likes
I had to ask AI to think about it as I’m too biased and possibly lazy thinker and it thinks that when “LEV” like singularity or AGI/ASI hits baseline health into it might still matter for treatments. You can’t really restore lost brain function, I mean like memory, as there won’t be enough precision in the restoration from prompt – unless the treatment fools someone just like a chair in a dream is what a chair looks like.
And because of LEV spectrum, maybe some things can’t really be reversed for a long time or fixed.
At least health might help with things radically changing.
LEV spectrum sounds like LED light spectrum, could be useful way to see it, like a rainbow, and it’s also artificial and a technology in some sense.
1 Like
New Scientist talks with Bryan Johnson:

1 Like
Blueprint is moving forward…
See full post here: https://x.com/bryan_johnson/status/1983196154490966322
3 Likes
Good ideas
1 Like
With AI one can write so much yet say so little.
6 Likes
On X Dr. Jack Schroder has a lengthy interesting critique of Bryan Johnson’s April 2025 labs.
Schroder vs. Johnson
Two points where I part ways.
First, LDL. Jack frames very low LDL as inherently problematic. My own LDL is lower than Bryan’s, intentionally so, and I’m comfortable with that given coronary risk context and outcome data from LDL-lowering trials. Observational associations between low LDL and adverse outcomes are heavily confounded and don’t translate cleanly to deliberate, monitored LDL reduction.
Second, IGF-1 and SHBG. Jack notes low IGF-1 and elevated SHBG and treats them as yellow flags. In my own case, E3 shifted both markers in the same direction as Bryan’s, without any obvious functional downside. These look like expected tradeoffs of certain longevity-leaning interventions rather than clear pathology.
Jack’s main concerns in the labs were:
• Low WBC and neutrophils
• Low platelets and globulin
• High SHBG
• Very low total cholesterol
• Low glutathione / GGT
• Low ferritin
• Low IGF-1
• Mild AST elevation←my ALT/AST are slightly better also, idkw
I’m not a doctor, and this stuff gets really confusing fast. But weighing the total picture, I still lean closer to Johnson’s interpretation than to the claim that these labs suggest hidden systemic breakdown.
(edit)
LatestJohnsonPost…Defensive?
He just now tweeted his HA1c results-super low. I don’t see how to jive this with the high blood glucose reading of 103 as I recall.
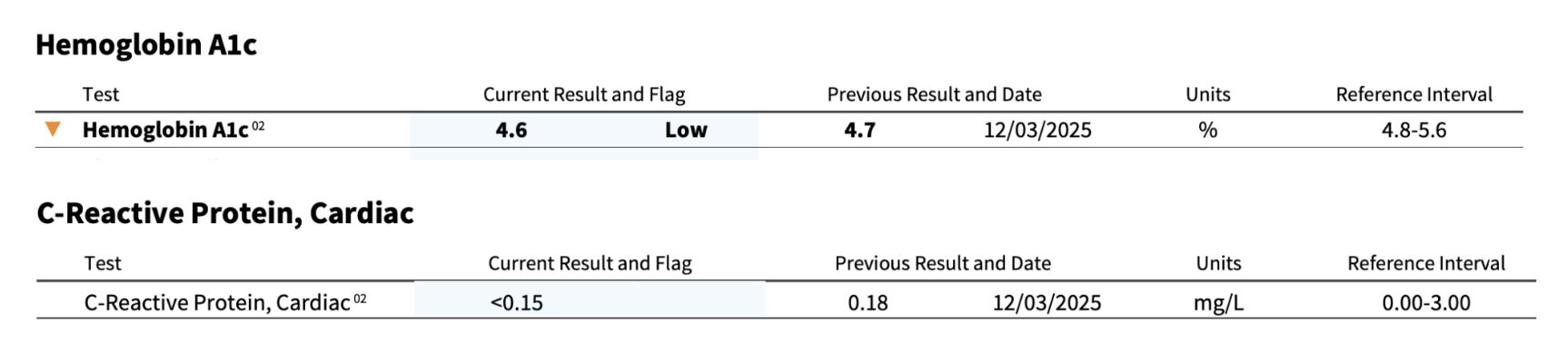
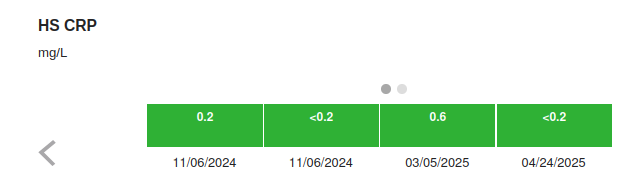
Also he’s rich, why wouldn’t he buy a high dollar hs-CRP? My poor boy $50 test gets down to 0.2. I think some labs have crp tests that go down to 0.10
(Last Edit)–The Mystery of the crushed A1c and spiked Glucose
I asked AI how you could have high blood glucose and super low A1c and got a list of possiblities, but #1 on the list???
Says AI:
If therapeutic phlebotomy / blood donation is in the mix and you’ve seen low ferritin plus hemoglobin shifts, then the A1c–glucose mismatch is no longer mysterious at all.
HbA1c is glycation over red blood cell lifespan (~120 days).
Phlebotomy:
- Removes older, highly glycated RBCs
- Forces marrow to make new, minimally glycated RBCs
- Shortens the average RBC age in circulation
Result:
- HbA1c drops, sometimes substantially
- Even if mean glucose does not drop proportionally
And the typical “tells” are:
Ferritin drifts low
Hemoglobin wobbles but stays “acceptable”
MCV may shift
RDW may increase slightly
A1c looks “elite”
This neatly explains the mystery, is it correct, IDK, but Johnson’s talked a lot about blood donations/transfusions and I seem to recall his ferritin was low and a few other slightly off blood markers
3 Likes
I’ve never heard of Dr. Jack Schroder…
I agree with parting with him on on the LDL issue. Heart disease is the number one killer of men, so I lower LDL agressively… and I follow the best, long term studies available, like this one: The Coronary Plaque Progression Paradigm: Why Your "Low Risk" Score Might Be Lethal
IGF-1, I’m more mixed on this issue, low IGF-1 is generally associated with longevity but the biggest impact is when the organism (mammal or otherwise) is very young, so if you have low IGF-1 in the first 10% of your life, you’re likely to live much longer (and be much smaller), but after that the benefit seems to be quite minimal. And there are (in talking with people who use it) many benefits to GH in terms of how you feel. So this may be a bit of a “quality of life” vs. “length of life” trade off that many people would side with on the “quality of life”, because the impact on total lifespan (if you’re looking at IGF-1 or GH levels after middle age) is not much of a factor.
3 Likes
Does anyone else believe Bryan is mistaken that science is to blame for hyperpalatable food?
I don’t think the foods that are enticing is Humanity’s first rodeo. Salt, sugar, and fat have been with us for a long time. Spices and processing as well.
The majority of the lifting was human ingenuity, cleverness, and trial-and-error over thousands of years.
Science did help make things cheaper and last longer. But the vast majority of impact it would be a stretch to claim it’s because of applied science. It’s more like chefs being chefs I think.
But scientists sounds more evil and more unnatural than chefs. There’s really no secret ingredients that makes us love hyperpalatable food. It’s base stuff!

2 Likes
When the Odyssey was written by Homer I am most certain there was some unhealthy food addicts.
Butter: 2500 BC
Salt: 6000 BC
Bread: 12000 BC
Sugar: 4000 BC
2 Likes