It’s probably a bit of both. A person can definitely make plenty of hyper palatable foods from scratch combining only basic things like flour, butter, sugar etc. and certainly chefs are experts at it. Our modern food environment has perfected doing this on a mass scale cheaply so now rich or poor we can easily consume the magical combination of salt, sugar and fat that gives us a dopamine hit all day everyday if we don’t know better. I thought this podcast was interesting in pointing out the connection of UPF’s with the tobacco industry.
2 Likes
And he makes the cover of Time magazine.
1 Like
Good to see him say this about LDL since a lot of people who pay attention to him get bombarded with “LDL is good” bad info.
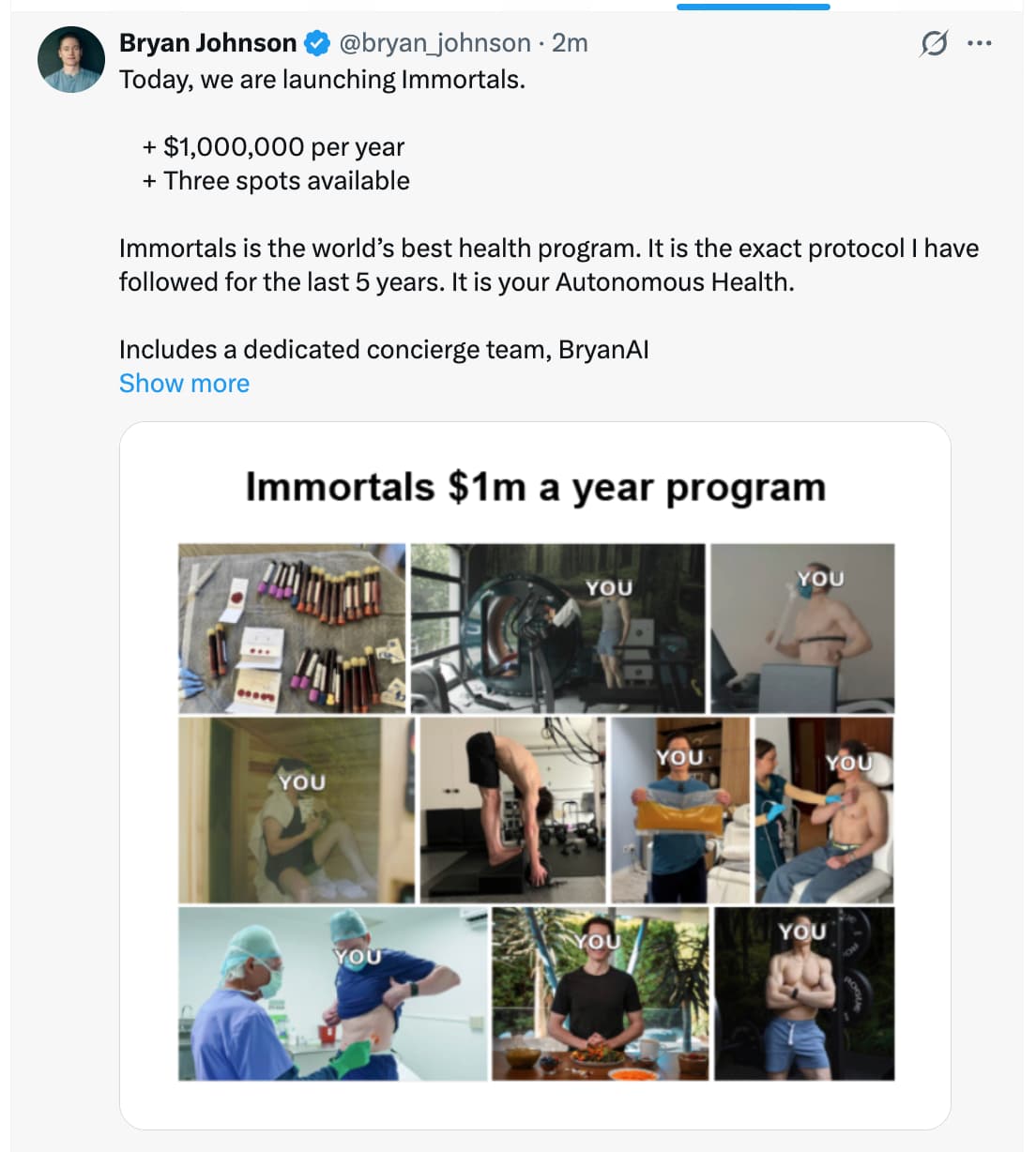
https://x.com/bryan_johnson/status/2008362857847812387?s=46
“Definitely do not stop statins, and preventative LDL-cholesterole lowering therapies in general, based on these arguments, as they clearly misrepresent the facts.
The AMORIS study only showed that extremely low total cholesterol was negatively associated with the chance of becoming a centenarian (reaching 100 years of age) (observational association; not causal, and low total cholesterol can also reflect underlying illness in older adults).
Total cholesterol is different from LDL. Statins specifically lower LDL in the blood by increasing LDL receptor expression in the liver.
The points made here perpetuate a common misconception, often propagated by health influencers, which is mixing up the beneficial functions of a molecule (nearly all naturally occurring biological molecules have legitimate functions in cells, tissues, and organs) with the level of these molecules in the blood, abnormally high levels do not mean a particular molecule is doing its job better, for a simple example, think of glucose, it fuels the brain, too much would not cause your brain to function more, the contrary as it causes metabolic disease, diabetes, and even increases cognitive decline risk.
Cholesterol, and even LDL, have their legitimate functions, but these functions do not improve when the molecules are abnormally high in the blood. In fact, elevated LDL in the blood is often an outcome of defective liver uptake, frequently due to metabolic disease, and in rarer cases, solely due to genetics (familial hypercholesterolemia).
LDL is causally linked to cardiovascular disease, and lowering it reduces heart attack risks in patients with existing plaque. Mendelian randomization studies also show that lifelong exposure to lower LDL levels reduces coronary artery disease risk; a 38.7 mg/dL reduction correlates to over a 55% reduction in coronary artery disease risk. Moreover, loss-of-function mutations in PCSK9 lead to a 28% reduction in LDL and correlate to an 88% reduction in coronary heart disease.
The genetic variants with lower cholesterol share a similar mechanism with statin or PCSK9 treatments, in that they mainly lower LDL by increasing liver clearance.
The U-shaped relationship between LDL-cholesterol levels and all-cause mortality at a population level is likely driven by reverse rather than actual causation, since many aging and chronic disease drivers, including inflammation, malnutrition, cancer, and liver disease, can all contribute to lowered levels of lipoprotein.
Contrary to the observational data, a large meta-analysis showed that more intensive statin regimens and further reductions in LDL cholesterol produced further reductions in heart disease events and death risk. 20% reduction in coronary heart disease death and 10% reduction in all-cause mortality per 1 mmol/L (38.7 mg/dL) LDL-C reduction across trials.
With that said, you might want to reconsider statins in the following cases:
A severely lowered LDL coupled with partially increased blood glucose can be a sign of cholesterol “overmedication.” The same mechanism that leads to increased clearance by liver uptake also works to increase LDL uptake by pancreatic islet cells. Preclinical evidence shows that overmedication to lower blood LDL can lead to disrupted pancreatic islet functions and insulin secretion, and increased blood glucose (In humans, statins are associated with a modest increase in diabetes risk overall; this is not reliably diagnosed by “LDL too low,” and risk is most evident in predisposed individuals).
Consider swapping to PCSK9 inhibitors. This is a well-established injectable (once every month or every two weeks) class of biologics (recombinant monoclonal antibodies targeting PCSK9 and preventing its effect in degrading the LDL receptors in the liver). PCSK9 inhibitors have shown added protective effects in lowering cardiovascular disease risk even in patients already on statins. They also have a speculative anti-aging mechanism since circulating PCSK9 has been shown to increase with aging. While they can also plausibly interfere with the pancreatic islets and cause similar disruption seen with statins, there is no evidence yet to date of PCSK9 inhibitors increasing diabetes risk, such as evidence exists for statins (major outcomes trials have not shown a significant increase in new-onset diabetes over ~2–3 years of follow-up).
If your HDL is too low, you need to pursue strategies to increase it, including exercise, healthy diets rich in MUFA and Omega-3 fats and fibers, avoiding added sugar and refined carbs, and abstaining (or seriously cutting down) on alcohol.
If you are experiencing muscle ache and discomfort with statins, this is also a strong reason to switch. While the more acute form of muscle degeneration is very rare and would have been detected earlier as you began your statin therapy, lower-grade muscle aches are common in statin users. Changing to PCSK9 inhibitors, or other medications like ezetimibe (a cholesterol absorption blocker), can also help.
Personally, I am currently on Repatha, a PCSK9 inhibitor, as I replaced statins after noticing they slightly increased my blood glucose.”
8 Likes
Update via email:
How I’m doing:

New protocols for 2025:
-
- sauna (link)
- magic mushrooms as a longevity therapy (link)
- metformin cycling (link)
- pulsed electromagnetic field (PEMF) therapy (link)
- intermittent hypoxia-hyperoxia therapy (IHHT) (link)
Graveyard protocols for 2025:
-
- SLU-PP-332: caused sleep disturbances (link)
- plasmalogens: didn’t do much for my biomarkers (link)
- methylene blue: made me less tolerant of IHHT, a potentially more beneficial protocol (link)
Our biggest discovery of 2025:
-
- I hit a metabolic reset switch with the psilocybin (magic mushrooms) therapy. This is a first-in-world observation in humans. More below, and a deep dive coming soon.
—————
Big breakthroughs:
#1… Magic mushrooms as a longevity therapy
We are testing 3 doses of magic mushrooms over 3 months. I’ve taken 2 doses, and we have already seen surprising results (watch).
The biggest breakthrough so far: Psilocybin may be a metabolic reset button for the brain. My blood sugar control improved from the top 2% of the population to 0.2%, better than 99.75% of 18-25-year-olds. I’ll share more data from our mushroom experiment in future emails, including more about our first in-human observations.
We think psilocybin is a longevity therapy.

#2… Skin age reversal of 9 years
I effectively froze my skin aging over the past 5 years.
-
- skincare: Blueprint cleanser, serum, and moisturizer
- diet and supplementation: Blueprint collagen peptides, flavonols, polyphenols (extra virgin olive oil), and antioxidant supplementation. My diet, which focuses on plant protein, fiber, and polyphenols, is also geared toward eliminating inflammation, oxidative stress, and glycation. All sources of skin damage.
- smart UV exposure: protect your skin when the UV index is high (10am - 4pm)
- skin-focused therapies: 1927-nm laser, 1550-nm laser, and Sofwave every 6 months
- whole-body therapies: daily red/nir light panels, hyperbaric oxygen therapy (HBOT), and dry sauna

#3… Sauna as a top longevity therapy
I started dry sauna in early 2025… and it turned out to be one of the most effective therapies I’ve done. I now do 20 min of sauna daily at 200°F (93°C). Clinical evidence for the temperature target in dry sauna is between 175°F and 212°F (79-100°C).
-
- 15 sessions of sauna dramatically reduced environmental toxins in my body
- my vascular function improved by a 10-year reduction in age
- sauna coincided with my fertility markers being at an all-time high (when I iced the boys)

#4… Eliminated 85% of microplastics from my ejaculate
Microplastics can invade organs, cross the blood-brain barrier, and wreak havoc with your hormones, fertility, and immune system. To reduce them, I tried to remove as much plastic from my life as possible.
Also, surprisingly, this year we discovered that sauna reduced microplastics in my blood and ejaculate by ~85%.
4 Likes
I’d love to read more about his experience with IHHT. For those interested we’re discussing IHT and IHTT here: Oxygen, hypoxia and hyperoxia
Bryan Johnson was on My View with Lara Trump, Feb 1, 2026.

I agree with Bryan Johnson. AG1/Athletic Greens are useless dreck. Just eat some salad.
7 Likes
Thanks for the heads up… only 2 spaces left… join me. Hahaha ![]() .
.
Changing my avatar to
Agetron
The Immortal Guy
Definitely has a better sound to it – I think.
7 Likes
![]()
![]()
![]()
![]()
![]()
![]()
![]() etc., etc.,…
etc., etc.,…
3 Likes
It’s actually brilliant because I bet there will be people who pay… having said that, I would not think they’d pay to only get Bryan “AI”… for Bryan, it would be an easier sell.
1 Like
My biggest fear if I joined - is that I’d start sending emails that say creepy stuff like:
“I go into BJ withdrawal when I don’t see him.”
Hmmm… those initials make it sound even more weird. ![]()
6 Likes
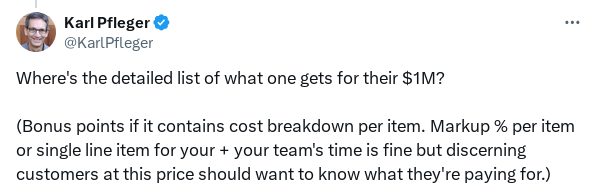
Mogged by Karl
5 Likes
Silly point scoring. With only 3 slots, they’ll probably sell out quickly, I reckon. Lots of people have that to throw around, crazy as it may seem. And frankly, you buy a Lambo and they don’t give you a cost breakdown or markup % per item. They offer it, you buy or don’t buy. Simple.
3 Likes
$1M a Year to Live Forever? Bryan Johnson Explains

I. Executive Summary
This transcript details the evolution of the “Blueprint” protocol from a public experiment into a commercialized, ultra-high-end longevity service called Immortals, priced at $1,000,000 annually. Bryan Johnson argues for a paradigm shift from “human-led” health to “Autonomous Health,” where AI-driven inference engines manage biological variables based on massive data acquisition (reportedly billions of data points per individual).
The core thesis rests on the aggressive mitigation of “self-harm” through the elimination of hundreds of “death-accelerating” variables (e.g., environmental toxins, poor sleep, ultra-processed foods) and the simultaneous optimization of “life-extending” pathways. A significant portion of the discussion focuses on high-polyphenol Extra Virgin Olive Oil (EVOO) as a caloric staple, claiming it functions as a “superfood” with systemic benefits. However, Johnson introduces a critical adversarial stance toward the “Organic” label, dismissing it as a marketing tactic that fails to account for a broader spectrum of environmental toxins like heavy metals and mold.
From a clinical perspective, the transition to the Immortals program represents an extreme application of “N-of-1” precision medicine. While the data density is unprecedented, the translational gap remains significant: much of the “signal” Johnson seeks to extract from his “inference engine” relies on unverified correlations that have not undergone rigorous, large-scale RCT validation. Furthermore, Johnson issues a rare safety warning regarding the “gray market” peptide industry, noting that while compounds like Tirzepatide are well-characterized, the broader class of “research” peptides lacks human safety data and clear side-effect profiles.
Ultimately, the protocol advocates for a “Don’t Die” ideology, prioritizing biological vibrancy as the primary human identity in an AI-dominated future. While the technological ambition is high, the reliance on bespoke concierge teams and proprietary AI limits the current scalability of these insights for the general population.
II. Insight Bullets
- Extra Virgin Olive Oil (EVOO) Staple: Consumption of 15–45 ml daily as a primary source of monounsaturated fats and polyphenols.
- The “Snake Oil” Rebranding: A strategic marketing irony used to emphasize ultra-rigorous, third-party molecular testing over vague health claims.
- Organic Label Skepticism: Organic certification is viewed as insufficient because it monitors a narrow subset of toxins, often ignoring heavy metals and environmental pollutants.
- Environmental Auditing: Prioritizing home inspections for mold, VOCs, water quality, and air toxins as a fundamental “Don’t Die” pillar.
- Autonomous Health: Moving away from “human driver” health decisions toward AI-led protocols that predict needs better than the individual.
- Data Density vs. Signal: Claiming a “dimensional representation” of a human through billions of data points, though only a fraction (millions) are currently actionable.
- Peptide “Blind Spots”: Acknowledgment that many popular peptides lack human clinical trials, creating high-risk “drug-like” effects without side-effect characterization.
- CO2 and Cognitive Load: Identifying CO2 levels >1,000 ppm as a direct trigger for impaired executive function and cognitive decline.
- Light Hygiene: Using specific photon counts and lighting environments at bedtime as a non-negotiable sleep optimization protocol.
- Incentivized Data Ecosystem: A theoretical future where individuals are paid by companies to access their high-fidelity longitudinal health data.
- Early Time-Restricted Feeding (eTRF): Shifting the caloric window to early in the day (e.g., 8 AM – 2 PM) to optimize sleep architecture and REM cycles.
- Inference Engine Limitations: Current supplement cycling and protocol adjustments still face “confounding” variables in N-of-1 experiments.
III. Adversarial Claims & Evidence Table
| Claim from Video | Speaker’s Evidence | Scientific Reality (Current Data) | Evidence Grade | Verdict |
|---|---|---|---|---|
| EVOO is the “superfood of superfoods” | Personal protocol / anecdotal stacking. | High-phenolic EVOO reduces inflammatory markers (IL-6) and improves lipid profiles. Gaforio et al., 2023 | A | Strong Support |
| Organic produce is “worthless” / high in toxins | Internal testing of fresh produce. | Organic foods have lower pesticide residues, but heavy metal contamination (Lead/Arsenic) persists across both types. Smith-Spangler et al., 2012 | C | Plausible (Partial) |
| Peptides have “drug-like” effects but lack safety data | General observation of the “Chinese peptide” market. | Many “research only” peptides (e.g., BPC-157) lack human RCTs for systemic safety. Wellenstein et al., 2024 | E | Safety Warning |
| CO2 > 1000ppm impairs thinking | Personal monitoring / HVAC work. | Elevated CO2 levels in indoor environments are proven to significantly reduce cognitive scores in office/classroom settings. Satish et al., 2012 | B | Strong Support |
| Early meal timing (eTRF) is superior | Personal 11 AM “dinner” protocol. | Early TRF improves insulin sensitivity and reduces 24-hour mean glucose compared to late TRF. Jamshed et al., 2022 | A | Strong Support |
IV. Actionable Protocol (Prioritized)
High Confidence Tier (Level A/B Evidence)
- High-Phenolic EVOO Supplementation: Incorporate 15–30 ml of high-quality EVOO daily. Prioritize oils with high oleocanthal and oleuropein content (noted by the “peppery sting”).
- Indoor Air Management: Maintain CO2 levels below 800 ppm. Use HEPA filtration to mitigate VOCs and particulate matter (PM2.5).
- Early Time-Restricted Feeding: Aim to finish the final meal 6–8 hours before sleep to maximize heart rate variability (HRV) and deep sleep.
- Blue Light Mitigation: Use amber-tinted glasses or eliminate screen use 2 hours before bed to preserve melatonin production.
Experimental Tier (Level C/D Evidence)
- Precision Peptide Use: Only use peptides with FDA-approved clinical histories (e.g., GLP-1 agonists like Tirzepatide) under medical supervision. Avoid uncharacterized “research” compounds.
- Home Toxin Auditing: Perform a comprehensive check for mold (ERMI test) and heavy metals in drinking water.
Red Flag Zone (Safety Data Absent)
- Unverified Peptide Sources: Procuring compounds from non-regulated “research” chemical suppliers (e.g., the “Chinese peptide meme”) carries significant risks of impurities and unknown long-term toxicity.
- Extreme Caloric Restriction without Monitoring: Risk of hormonal suppression (low testosterone) as mentioned in the anecdotal case in the transcript.
V. Technical Mechanism Breakdown
- Oleocanthal-Induced Autophagy: The “sting” in olive oil is caused by oleocanthal, a natural phenolic compound. Mechanistically, it acts similarly to ibuprofen as a non-selective COX inhibitor but also modulates mTOR signaling, potentially inducing autophagy and clearing senescent cells.
- Cognitive Carbon Dioxide Toxicity: Elevated CO2 acts as a mild narcotic. It alters the pH of the blood (respiratory acidosis), which can shift oxygen-hemoglobin dissociation and impair cerebral metabolic rates of oxygen consumption (), leading to the “brain fog” described.
- Circadian Entrainment via eTRF: Feeding serves as a “zeitgeber” (time-giver) for peripheral clocks in the liver and gut. Early feeding aligns these peripheral clocks with the master clock (SCN), reducing metabolic friction and Improving glycemic variability.
- AI Inference Engines in Biology: Johnson’s “Inference Engine” likely utilizes multimodal deep learning to find non-linear correlations between disparate data sets (e.g., photon counts at night vs. morning HRV). This aims to solve the “curse of dimensionality” in biology where traditional statistics fail.
1 Like
If you’ve been following him, you know exactly what you will get for your $1,000,000. Exercise. Nutrition, sleep, psychedelics and buy his supplements.
A fool and their money…
6 Likes
Blood tests, HBOT, sauna, and probably a bit more. Overpriced though.
2 Likes
Gil Carvalho Reacts to Bryan Johnson´s Bloodwork

5 Likes