It’s interesting and it made me think about buying more niacin and just selling my extra NNN-C, but maybe the NMN-C might be absorbed into the muscles (but still into other tissue)
Tbf he lost a little credibility to me after his anti-metformin video (which I also found to be a bit sexist)
Since you care about influencer opinion so much, even Barzilal, a huge proponent of metformin, who is often cited here trying to push all these metformin studies does not recommend to take metformin when age<40.
Can you explain what makes Stanfield biased and “sexist”? Upon a quick look, he appears to have taken metformin 1 year ago and claimed he got “sucked into hype”. He appears to be citing older adults shown to have huge blunt in exercise effects again in human trials. I had the same concerns earlier on top of the issue with ITP null results with monotherapy.
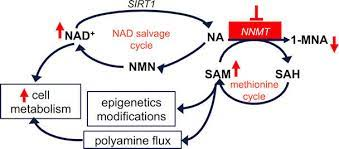
As for NMN/NR/other proponents, I’ve yet to see any mention of NNMT part of the pathway or its inhibitors. As far as I can tell, no career researchers who are proponents have really mentioned this pathway:
He’s super-conservative in being anti-experimentation, he has reputation points to lose (he already has to be on the defensive for advocating metformin for non-diabetic individuals so in advising against metformin for under 40-year-olds he is OVERCORRECTING so that he does not appear too extreme [and has less surface area for “attack”), I don’t consider him a credible source on this. In general, society benefits when people self-experiment more.
Can you explain what makes Stanfield biased and “sexist”?
He says it lowers testosterone levels as a reason NOT to take it. This is (mildly) sexist against women and transgender individuals (not to mention that testosterone ITSELF is pro-aging)
I have intense anger towards testosterone for giving me “girl issues” that have cost me 3-4 years out of my life. AND testosterone is shown to increase epigenetic aging rate
Not sure how that is “sexist”. It seems you’re defaulting to an assumption of malice.
Is claiming any medication lowering estrogen levels sexist as well? All types of sex hormones are present in each biological sex at different levels. A well classified syndrome of androgen excess in women is PCOS, such that “lowering testosterone” may be partly why we use metformin for PCOS beyond decreasing hepatic glucose production as a major effect.
As another example, testosterone reduces over time in aging women. Most of the testosterone are aromatized to estrogens in women, so lower testosterone may translate to lower estrogen levels as well. That may be of relevance for those of any gender. Even “low estrogen” which can be due to “lower testosterone” can become problematic in men. Estrogen isn’t unique to biological women and testosterone isn’t unique to biological men. Both hormones have functions for all genders and it is common knowledge in medicine.
From my observations, I quote your statement “f*** testosterone”. I think that may be the real issue here.
I said “a little sexist”. Sins of omission can be slightly sexist even if they have no malice (this is also mostly due to prevailing social messages - women tend to know/assume that way more medical advice is directed towards men than to women)
[fwiw I’m also pretty hypersensitive to sexism in the other direction, esp as it pertains to cancel culture and how it interfaces with both ageism and status - I know full well that the most discriminated-against-group is “low status older men”]
You haven’t really explained how that is a sin of omission. Where did you find out that Brad Stanfield knows what you define as “good behavior” is “good”? He cannot commit a sin of omission if he doesn’t know of whatever “good” you’re talking about.
You appear to be assuming he is willingly committing a sin of omission in asserting what appears to be a neutral statement until otherwise provably not, due to willingly not performing some “good behavior” (as defined by you) with knowledge of what that “good behavior” is. However, there is no evidence of whether he knows of whatever “good behavior” you are asserting as far as I can tell.
“This drug lowers testosterone levels” is a neutral statement. There is no reason to believe that his video was directed at males only. “This drug lowers estrogen levels” is also neutral. I’m not sure where he indicated or even implied that his audience is intended for males only or even mainly. Is it merely your perception of it being “a little sexist”?
Alex continues to raise a very important issue. Any discussion of longevity needs to consider issues of suicide, depression, and substance abuse. This is a much bigger deal than just girl issues. While I applaud Alex for raising the issue, I don’t think the consequences of testosterone are really Brad Stanfield’s job. Analogously, is a pill for obesity really the solution in a society drenched with high fructose corn syrup? Some issues are more moral, and cultural rather than medical. F. Roger Devlin is one of very few people writing about the family formation problem in an intelligent way. Monogamy is all but dead and has been replaced by rotating polyandry, or serial polygamy, or whatever you want to call our increasingly dystopian culture. Reducing testosterone might help some individuals to cope, but it does not solve the problem since society needs children in order to continue. If Brad Stanfield is a bit insensitive regarding these matters, perhaps he should be forgiven. He is not a President, Prime Minister, or Pope.
I don’t get the logic of Brad Stanfield. Sometimes it feels like he just wants to disprove Sinclair. Why is he strongly against NMN but still open for NR (Charles Brenner) and still taking niacin?
From my perspective, Stanfield is one dimensional. He is all about lifestyle, exercise, long term fasting and maybe soon Rapamycin. That’s a good start, but won’t save us. He works in a clinic with average sick people and is not a researcher. Good for the patients, but our focus is optimized, healthy people.
How can one know with accurately evaluated high certainty what is “optimal”?
The base rate of success is extremely low with clinical trials to FDA approval or even enough evidence to potentially warrant off-label.
It doesn’t seem like he’s completely against people taking NMN. Frankly, what I got from it is his claim is historically some NMN supplements have poor quality or even no NMN in them and with the potential legal issues raised with Sinclair’s FDA drug application - it would be reasonable to be wary how legit the average supplement company currently selling NMN is.
I personally have repeated that regardless of NMN/NR/other camp one is in - it seems that NNMT is disregarded despite being a big potential part of the NAD pathway - which smells to me that the lack of address seems to be due to bias and over-optimism across the board. Fact is NR monotherapy was a dud for extending lifespan in the ITP. I have serious doubts NMN or NA would on their own either.
Lowering testosterone in either biological sex can be an issue. Women with low testosterone levels (relative to normal female range) end up with many of the same issues that men with low levels do. While the normal levels for each are different, going below the standard range results in similar problems.
I do agree that Dr Stanfield is usually very conservative and does not like to recommend anything that doesn’t have very solid human data. That is an unimpeachable threshold for evidence, but most of us here are ok with pushing the threshold lower if there is reason to believe safety and benefit.
That said, he is spearheading a small human trial involving rapamycin. Which is interesting but also a bit confusing to me. He is looking at muscle performance in older people. I was not aware of that being a key effect of rapamycin, increasing muscle performance.
Funny, but there is a place for success stories and selfies as a means of encouraging others. Dennis Mangan was such an influence for me. If we add categories to these forums we should consider a success stories section. I’d prefer to keep the rest of the site more objective lest it turn into facebook.
I also think he lost a little credibility to me after the anti-metformin video. In particular I think his comment about testosterone is not warranted for two reasons. Firstly metformin can’t really be reducing testosterone to a considerable amount in most people because if it did it would have been known information for long since metformin has been used by decades by millions of humans. The fact that nobody noticed a reduction and none was seen in various studies suggests that it’s at best a very small effect. Secondly, even if metformin would reduce testosterone slightly in some people, that’s not necessarily harmful. In many young men that already have high testosterone, a slight reduction might do more good than harm. I don’t think the potential tiny lowering of testosterone in some people is a reason to not take metformin except for in some exceptional cases.
")