Drawing on nearly 400,000 UK Biobank participants tracked for over 15 years, this study reports that people who eat processed meat most often develop gout at modestly higher rates than those who rarely touch it — an association that survives adjustment for socioeconomic status, overall lifestyle, and a battery of clinical covariates. Machine-learning models ranked processed meat as the single most influential behavioral factor for gout, and a plasma-proteomics arm identified 40 circulating proteins tying diet to disease through metabolic, inflammatory, and neuroendocrine pathways. The headline twist: the risk gradient was steepest among the socioeconomically disadvantaged, reframing gout as a disease of inequality rather than aristocratic excess.
Gout has an image problem. For centuries it was the “disease of kings” — a punishment for port, venison, and rich living. This large prospective analysis of UK Biobank data argues that the modern reality is almost the inverse: gout is increasingly a burden of the poor, and one of its contemporary drivers may be the cheap, industrially processed meat that fills budget shopping baskets.
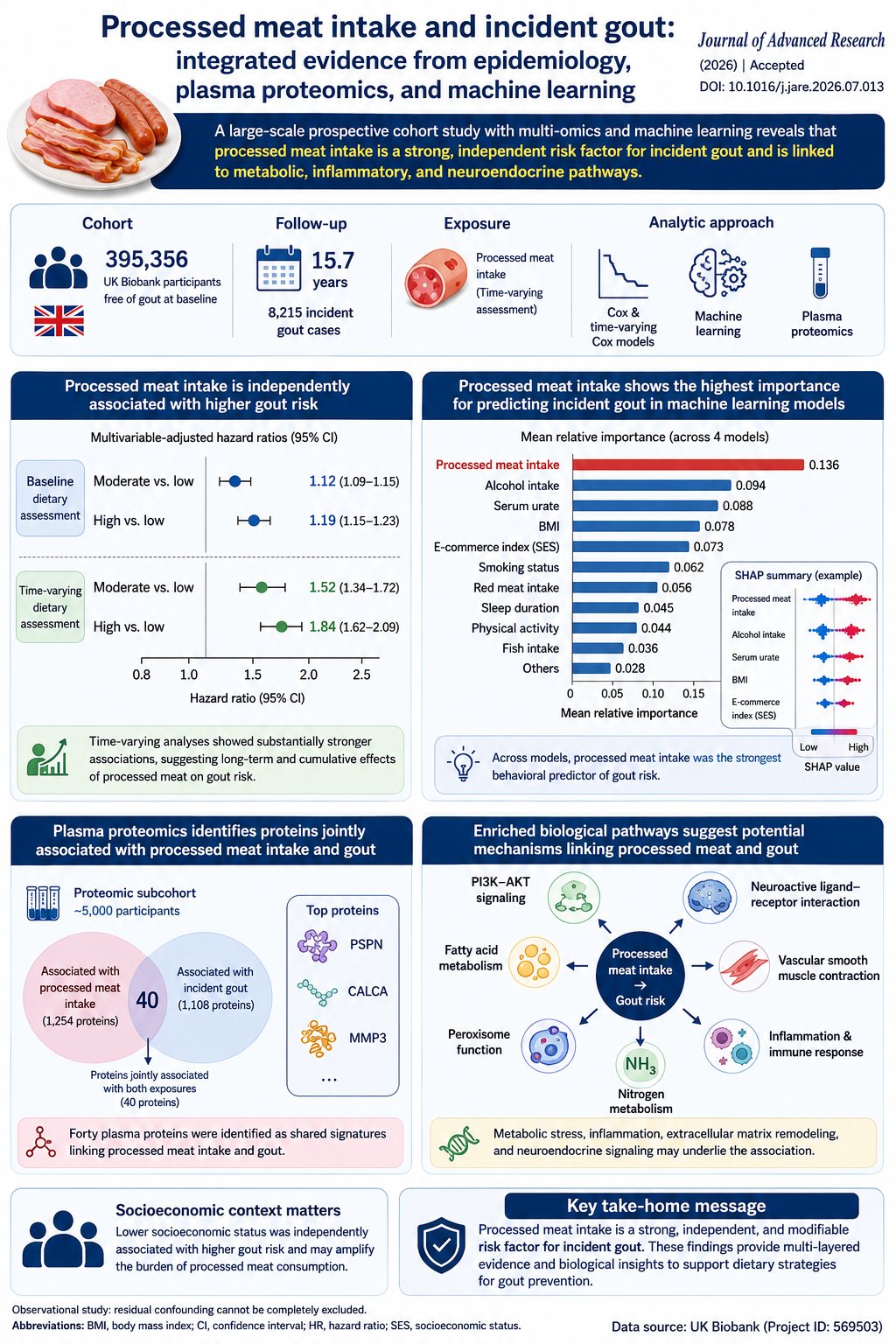
The researchers followed 395,356 gout-free adults for an average of 15.7 years, during which 8,215 developed the condition. After stripping out the effects of income, education, employment, smoking, alcohol, sleep, physical activity, body weight, kidney function, and other diet, people eating processed meat most frequently still carried roughly 19 per cent higher odds of incident gout than those eating little to none. When the team tracked people’s changing diets over time rather than relying on a single baseline snapshot, the estimated risk climbed further — an 84 per cent relative increase for the heaviest consumers, though with considerable statistical uncertainty.
The more provocative finding is about who pays. At identical levels of processed-meat consumption, participants of lower socioeconomic status developed gout more often than their wealthier counterparts. The authors argue this reflects a convergence of chronic stress, delayed diagnosis, poorer management of coexisting metabolic disease, and reduced healthcare access — structural forces that appear to lower the biological threshold for inflammatory disease.
To probe mechanism, the team measured almost 3,000 plasma proteins and isolated 40 that were jointly linked to both high processed-meat intake and subsequent gout. These clustered in pathways governing fatty-acid metabolism, insulin-like signaling, and — intriguingly — neuroendocrine and pain-related signaling, including the neuropeptide CGRP. The suggestion is that processed meat may prime a low-grade metabolic and inflammatory state years before a first flare, well beyond the classic purine-uric-acid story every gout patient is told.
The caveats are substantial: this is observational, diet was self-reported, purine intake could not be measured at all, and the proteomics is explicitly exploratory. No one should read this as proof that a ham sandwich causes gout. But as a signal that dietary guidance should treat processed meat as its own category — and that prevention should be aimed hardest at those least able to absorb the risk — it is a useful contribution.
Actionable Insights
The message is modest but real: processed meat appears to raise gout risk on its own, not just because people who eat a lot of it tend to have unhealthy habits in general. Even after the researchers accounted for those other habits, the heaviest processed-meat eaters were about 19 percent more likely to develop gout than people who rarely ate it. Moderate eaters were about 12 percent more likely.
Practical points:
- Distinguish processed from unprocessed meat. The paper argues (and its data support) treating cured/smoked/industrially processed meat as a discrete exposure rather than lumping all “meat” together. Red meat was adjusted for separately and processed meat remained significant.
- The urate pathway still dominates. Mediation analysis showed serum urate carried much of the (already small) processed-meat signal — for middle intake, the indirect (urate-mediated) HR of 1.07 exceeded the direct HR of 1.04. Urate-lowering behaviors and drugs remain the highest-leverage intervention.
- Context multiplies risk. The effect was strongest in low-SES strata, implying that reducing processed-meat intake yields disproportionately larger absolute benefit in metabolically vulnerable, high-baseline-risk individuals.
Context / Source
- Open Access Paper: Processed meat intake and incident gout: integrated evidence from epidemiology, plasma proteomics, and machine learning
- Authors/Institution: Wang, Shi, Pan, et al. — The Orthopaedic Medical Center, Second Hospital of Jilin University, Changchun, China (with Queen Mary University of London). Data: UK Biobank.
- Journal: Journal of Advanced Research (Elsevier, on behalf of Cairo University). Pre-proof, accepted 2 July 2026.
- Impact Evaluation: The impact score of this journal is 13.0, therefore this is a High impact journal