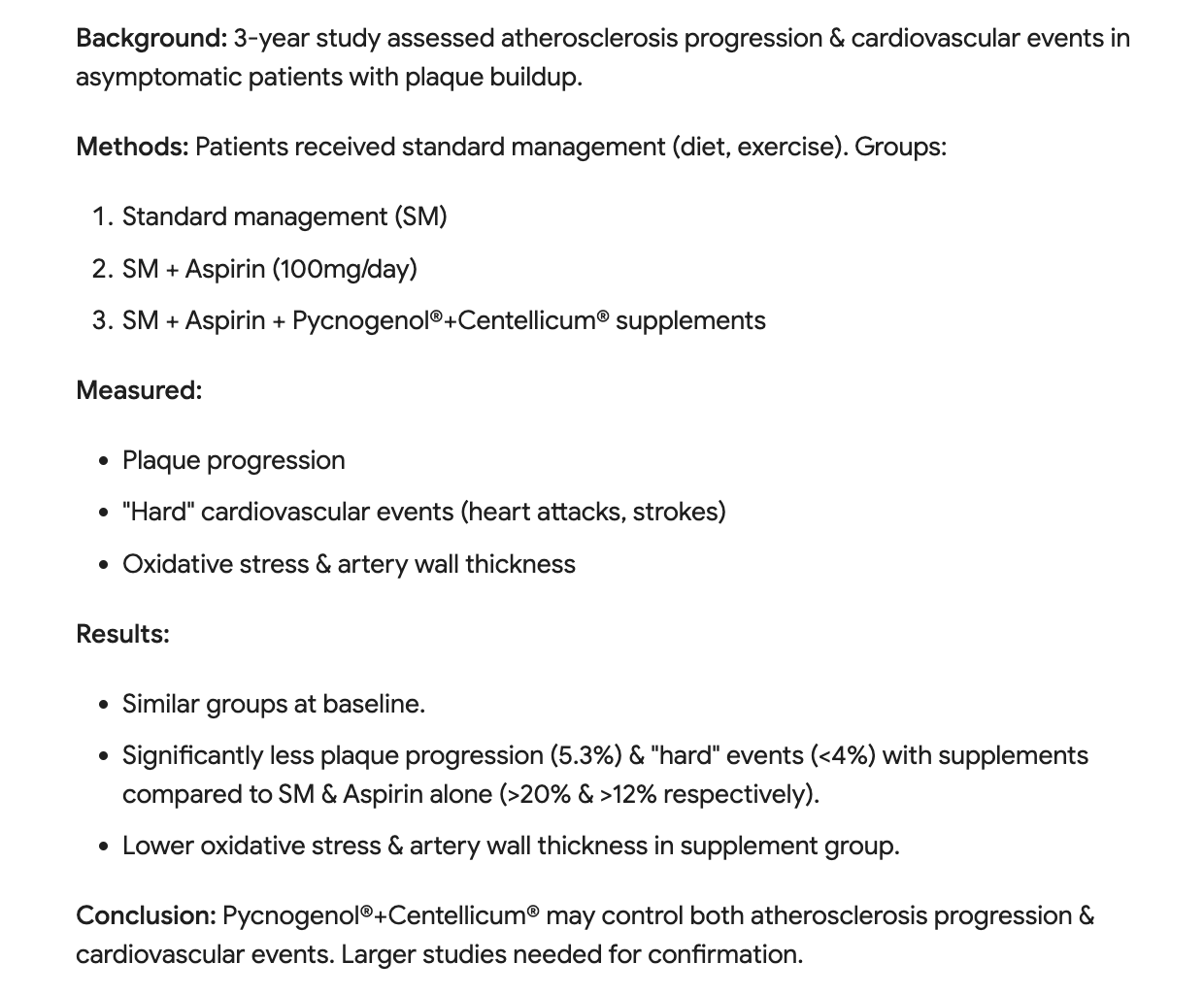
Aspirin + Pycnogenol + gotu kola = Reduced Plaque Progression: 5% vs >20% in others (statistically significant).
2019 https://pubmed.ncbi.nlm.nih.gov/31625707/
Aspirin + Pycnogenol + gotu kola = Reduced Plaque Progression: 5% vs >20% in others (statistically significant).
This recent trade publication on pycnogenol contains some interesting information (claims). I have been taking pycnogenol for at least 10 years, usually 100 mg/day and often with Gotu Kola. My rationale is evidence-based and my main target is arterial health. Based on the research, it could also be one of several supplements I take that contribute to my very low hsCRP. I don’t know that I can attribute any specific behavioral effects to this supplement.
Pycnogenol - Cognitive Function at any age_2024.pdf (910.8 KB)
effects to pycnogenol.
Is that better than plaque regression, achieved by keeping ldl under 55 for 1-2 years?
The study is unfortunately paywalled… so hard to evaluate the claims. I’ll try to get a full paper. But it sure looks like an industry-funded paper, which makes me suspect its not as rigorous as you would want.
Since the plaque stabilization/regression induced by pycnogenol+Gotu kola would be through an anti-inflammatory mechanism, it should be additive or even potentially synergistic with the effect of keeping LDL/ApoB at very low levels.
There are tons of claims of plaque regression for various interventions, and associated studies. The most recently highlighted by online health content creators are garlic extract (and aged garlic), and lutein + lycopene. These various interventions are cyclically in the news, and they become hot for a moment, then it’s on to the next one. Take your pick.
Ok, but any cyclic popularity is unrelated imo to their effectiveness or lack thereof. All we have is whatever studies we have.
It would be, if they were both used at the same time. But if I had to choose one, seems like keeping ldl low would provide more benefits.
When it comes to atherosclerosis, I certainly wouldn’t just choose one or the other when it comes to lipids vs inflammation. The major medical cardiology groups are finally acknowledging what most of us have known for years/decades (brief summary from OpenEvidence):
The American College of Cardiology recently acknowledged inflammation as crucial in cardiovascular disease through a 2025 scientific statement that declares “the evidence linking inflammation with atherosclerotic CVD is no longer exploratory but is compelling and clinically actionable” and states “the time for taking action has now arrived”.
The American College of Cardiology emphasizes that chronic, low-grade inflammation plays a crucial role in both the pathogenesis and clinical outcomes of cardiovascular disease. The statement highlights that residual inflammation, measured by high-sensitivity C-reactive protein (hsCRP), remains strongly predictive of recurrent events even in statin-treated patients, and elevated hsCRP in apparently healthy individuals identifies higher-risk groups who benefit from statin therapy even when LDL cholesterol is normal.
The organization’s rationale centers on robust evidence from randomized controlled trials demonstrating that targeting inflammation reduces cardiovascular risk independent of lipid lowering.
From post 20 by rivasp12
Rapamycin and risk of cardiovascular disease - #20 by rivasp12
“See article by cardiologist Joel Kahn MD to prevent and or reverse CAD with simple combination of gotu kola with pine bark extract . Scroll to page 37:”
My Clinical Practice
I spent seven years after medical school completing my training in interventional cardiology or using catheters to treat heart disease. Much of my practice involved inserting stents to prop open coronary arteries that were occluded with atherosclerotic plaque.But three weeks into my first job, I decided there was a better, more comprehensive approach. At that time, I read a study in a respected medical
journal focusing on atherosclerosis, which often leads to heart attacks and strokes. The study reported that atherosclerosis had been reversed using lifestyle and diet changes.2 Since then, I’ve combined interventional cardiology with a search for lifestyle and supplement-based methods to stabilize and reverse plaque buildup.I was particularly impressed by a published study that reported on a combination of extracts of French > maritime pine bark and an herbal extract called Centella asiatica. When added to standard diet, exercise, and lifestyle counseling, these two plant extracts improved plaque stability and reduced size and numbers of arterial plaques. The study involved 50 patients with plaque in the carotid arteries, which supply blood to the brain, neck, and face. These patients had no history of cardiovascular events, and did not have diabetes or metabolic problems.1 Over the three-month study period, pine bark + Centella asiatica extracts reduced carotid artery plaque and lowered the number of plaques compared to a control group.
After these scientific findings were published, this pine bark-Centella extract combination became a routine part of my atherosclerosis reversal program.
The Evidence Mounts I grew more convinced of the effectiveness of this plant combination when a larger, longer-term study was published in 2017. 3 This time, 391 subjects were followed for four years. All had asymptomatic atherosclerosis of either the carotid artery or the femoral artery (which provides blood to the leg). Atherosclerotic lesions extended 50%-60% into the arteries in at least one location. Three treatment groups were formed. One was treated with extract of pine bark alone, another was treated with pine bark and Centella asiatica, and a third control group received no extracts. All groups received standard diet, exercise, and lifestyle counseling. The rate of plaque progression, measured by ultrasound, was significantly lower in both treatment groups than in the control group. The group that took the combination of the two extracts had the greatest reduction in progression of plaque thickness and length.
The extracts also had a favorable impact on cardiovascular outcomes as follows:
• The occurrence of angina, chest pain caused by reduced blood flow to the heart, was less
than 3% in the two extract groups, compared with 6.25% in control patients.• The rate of heart attacks was significantly lower for the combination therapy.
• Events requiring hospital admission occurred in 16.4% of control subjects, 8.9% of subjects
using only French maritime pine bark extract, and just 3.3% of patients using the combination of pine bark and Centella extracts.
There is more. Just read the pdf.
Old post but since ASCVD is one of my risk factors, I try to stay abreast and evaluate emerging research. Based on my composite understanding and within normal ApoB bounds, I would not place it above arterial inflammation as longevity factors pertaining to arterial health. Better to optimize both, of course but it could be empirically superior in some cases to focus more on inflammation than reducing ApoB. (I shifted to ApoB because LDL-C does not appear to be destructive of arteries whereas ApoB is.)
If this study is truly critical, I’d be happy to try and buy the full paper for the group. However, to be honest, I haven’t seen any strong evidence in this thread so far showing why Pycnogenol is so important.
I’ve taken a look at some of the research on Pycnogenol, and honestly, I don’t see much value in this compound. Even regular anthocyanins seem more than enough to replace it.