They have a lot of omega-6, but also a lot of anti-inflammatory nutrients…
But linoleic acid makes its way into human tissue
They have a lot of omega-6, but also a lot of anti-inflammatory nutrients…
But linoleic acid makes its way into human tissue
studied the fatty acid compositions of the almond oil and found palmitic (0.39%), palmitoleic (0.56%), stearic (1.20%), oleic (71.98%), linoleic (20.37%) acids as the main fatty acids in almond oil.
All I know is that my CRP was 0.03 a day after I ate 2500 calories of almonds last year…
I guess judging by the above study that your genes and almonds are a good marriage.
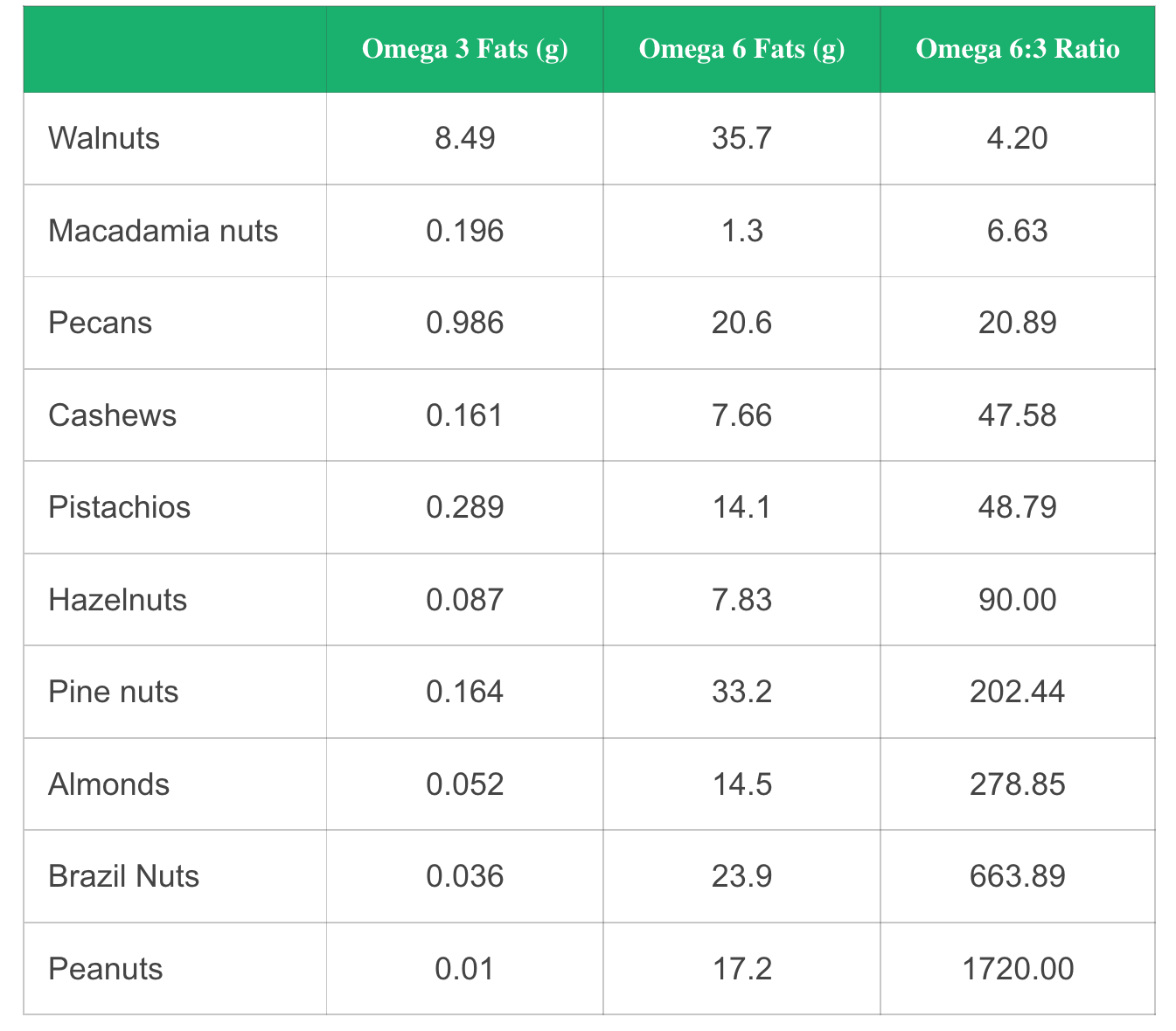
Most all of the literature I’ve read, is you want to keep your OMEGA 6:3 ratio less than 4:1.
Look at peanuts, America’s favourite nut…pretty much 100% omega-6.
I avoid all seed oils, and only consume EVOO (although it has omega-6). I try to get my omega-3 from whole foods, and select nuts (no peanuts, little almonds, mainly walnuts, macadamia, pecans, pistacchio). I do take 3 g/day DHA/EPA fish oil. After 6 yrs on this diet, my hsCRP is near zero, and my last OMEGA3 index was almost 12%. Omega 6:3, 3.98.
From the Harvard Health link you provided:
“The latest nutrition guidelines call for consuming unsaturated fats like omega-6 fats in place of saturated fat (hmmm…need to fact check this). The AHA, along with the Institute of Medicine, recommends getting 5% to 10% of your daily calories from omega-6 fats. For someone who usually takes in 2,000 calories a day, that translates into 11 to 22 grams. A salad dressing made with one tablespoon of safflower oil gives you 9 grams of omega-6 fats; one ounce of sunflower seeds, 9 grams; one ounce of walnuts, 11 grams. Most Americans eat more omega-6 fats than omega-3 fats, on average about 10 times more. A low intake of omega-3 fats is not good for cardiovascular health, so bringing the two into better balance is a good idea. But don’t do this by cutting back on healthy omega-6 fats. Instead, add some extra omega-3s” More hmmm…
I’ve heard pumpkin seed oil is healthy. Does anyone know anything about that or black seed oil (cumin)?
Why the Omega-3/Omega-6 Ratio May Not Matter After All | Mark's Daily Apple I was under the impression that the ratio of omega 6 & 3 not important anymore.
Lipofuscin levels are also affected by pro-oxidants and antioxidants in the diet (Katz et al., 1978). These authors have shown, using the retinal pigment epithelium of rats, that high levels of polyunsaturated fatty acids and/or low levels of antioxidants produced higher levels of lipofuscin. The accumulation was small in animals fed with a normal balanced laboratory diet. Katz et al. (1984) has also shown that the increase in lipofuscin due to antioxidant deficiency, vitamin E in this case, was not the same in all tissues. Using mice, these authors verified that increased accumulations could be observed in the retinal pigment epithelium, uterus and duodenum, but not in the spinal cord and some brain areas, while older animals fed a normal diet showed lipofuscin accumulation
Intervention trial showing inflammatory response to dietary linoleic acid depends on your fads1 (D6D) genotype. D6D limits conversion of LA to oxylipins. Supplemental has detailed listing of oxylipins. Supplemental: https://ars.els-cdn.com/content/image/1-s2.0-S0002916522030933-mmc1-sup1-s7.zip… Paper: https://sciencedirect.com/science/article/pii/S0002916522030933?via%3Dihub…
==
also see the image I just posted on MUFAs thread…
The journals say that PUFAs reduce heart disease and mortality risk even more than MUFAs, but does this account for most PUFA consumption in america often being in the form of highly processed seed oils, often rancid/damaged because food has been fried in PUFAs
Below is a “road-map” of the metabolic traffic-lights that decide where the linoleic-acid (LA, 18:2 n-6) you eat ends up—either shunted toward pro-inflammatory arachidonic acid (AA) and eicosanoids or steered into more neutral/beneficial fates. For each step I list the rate-limiting enzymes, common functional polymorphisms, and what we know about their diet-gene interactions, disease links, or longevity signals.
| Pathway step | Gate-keeper genes (enzyme) | What the key variants do | Why they matter for inflammation / longevity |
|---|---|---|---|
| 1 · Desaturate + elongate LA → γ-linolenic acid (G LA) → dihomo-γ-linolenic acid (DGLA) → AA | FADS2 (Δ6-desaturase) & FADS1 (Δ5-desaturase) sit back-to-back on chr 11q12; ELOVL5 / ELOVL2 add the two-carbon “spacers” | “Derived” haplotype (rs174550-T, rs174546-T, etc.) gives ↑ Δ5/Δ6 activity → higher AA / lower LA; “ancestral” haplotype does the opposite. Enzyme activity differences can exceed 50 %. (PMC, ScienceDirect) | High-activity alleles amplify AA-eicosanoid output when LA intake is high, raising CRP, IL-6 and CAD risk; low-activity alleles look protective in modern seed-oil diets yet were selected against in populations where AA is critical for early brain growth. |
| 2 · Liberate AA from membranes | PLA2G4A (cPLA2-α) and secretory PLA2s | Coding SNPs (e.g., rs12746200-G) or promoter variants can dampen PLA2 activity → less free AA available to COX/LOX (PMC, ScienceDirect) | Reduced PLA2 function associates with lower MI risk and milder inflammatory responses. |
| 3 · COX branch: AA → prostaglandins / thromboxanes | PTGS1 (COX-1), PTGS2 (COX-2) | Rare coding SNPs; more commonly, COX-2 promoter −765 G→C lowers enzyme induction and PGE₂ output | PGE₂ drives tumorigenesis & immunosuppression; lower-induction genotypes link to slower CAD and colorectal-cancer progression. |
| 4 · LOX branch: AA → leukotrienes & HETEs | ALOX5 (5-LOX) + ALOX5AP (FLAP) | ALOX5 Sp1 promoter repeat: <5 repeats attenuate gene transcription → ↓ LTB₄ / cysteinyl-LTs; ≥6 repeats do the reverse (PubMed, PMC) | High-expressor genotypes heighten asthma, atherosclerosis, ischemic-stroke and shorten telomeres; benefit more from 5-LOX inhibitors. |
| 5 · CYP450 branch: AA (or LA directly) → epoxy- and hydroxy-oxylipins | CYP2C8/9, CYP2J2 epoxygenases make anti-inflammatory EETs / EpOMEs; EPHX2 (sEH) hydrolyzes them to pro-inflammatory diols | Common K55R and R287Q in EPHX2 raise sEH activity → ↑ DiHETEs / DiHOMEs, ↓ protective EETs (ScienceDirect, PMC) | High-sEH genotypes link to earlier MI, stroke, metabolic syndrome; sEH inhibitors extend lifespan in mice & improve vascular aging. |
| 6 · Peroxidation / clearance of oxidised LA (OXLAMs) | ALOX15 / ALOX12, GPX4, GSTP1, NQO1, NRF2 | Variants that blunt antioxidant enzymes allow oxidised LA metabolites (9- & 13-HODE, 9–KvA) to accumulate | Elevated OXLAMs predict frailty, dementia and shorter lifespan in several cohorts. |
“Two knobs” set your personal AA tone
Why seed oils look “pro-longevity” on average
How to tell which side you’re on
| Biomarker / test | What it indicates |
|---|---|
| Genotype panel for FADS1/2, ELOVL5, ALOX5 Sp1 repeats, EPHX2 K55R | Fixed “upper-pathway” capacity |
| Plasma AA : LA ratio & oxylipin panel (EETs / DiHOMEs, 9-HODE, 13-HODE) | Real-time balance between pro- vs anti-inflammatory flux |
| Urinary PGE-M & LTE₄ | COX / LOX throughput |
Diet tweaks that interact with genotype
Whether LA is a mild geroprotector or a stealth inflam-accelerant hinges on a “polygenic valve system.”
Genotyping (or at least checking your AA : LA ratio plus oxylipin fingerprints) gives actionable insight into whether dialing back seed-oil LA, upping ω-3s, or targeting sEH/LOX specifically will shift your personal balance toward healthier, longer-lived biology.
I have been eating pistachio nuts since provided as a bar snack in Greece. Countryside full of pistachio trees as far as you can see. They are a great food source for protein fiber and healthy fats.
Americans go nuts for ancient snack as expert weighs in on health perks, pitfalls