I think acarbose works more immediately, while SGLT2 inhibitors take some more time to work?
[it’s impt b/c sometimes I’m too impatient to eat]
I think acarbose works more immediately, while SGLT2 inhibitors take some more time to work?
[it’s impt b/c sometimes I’m too impatient to eat]
Yes, acarbose is faster and much more effective if you’re comparing just one dose of each. The SGLT2 inhibitors are meant as a once daily chronic dose where the medicine reaches steady state and increases glucose excretion 24/7. They aren’t meant for acute dosing like acarbose, which of course works almost immediately but just for that particular meal.
Yes - I use them the same way. On days when I don’t take the SGLT2i medication, I take acarbose if I’m going to be eating a starchy / higher carb meal - taking it at the start of the meal. That covers you.
Just don’t eat bread.
I only use acarbose prn for convenience purposes.
There are enough potential problems with monotherapy acarbose over the long run in real-life humans that people are too quick to jump on - so I use mostly traditional Okinawa diet instead.
Look at the microbiome analyses in Okinawan centenarians and what Okinawans actually eat/drink and you’ll see what I mean.
Possible infectious disease adverse effects (even if rare) of SGLT-2 inhibitors deter me from thinking about it (ie genital infections/cellulitis/Fournier’s gangrene). Happy to be proven wrong but the risk factors for Fournier’s gangrene in healthy individuals plus the other interventions typically used in “anti-aging” is significant and an extra thing like an insect bite plus neutropenia when in the context of glycosuria can tip the scales.
There are just other ways than dumping sugar in the urine to get similar effects for “healthy” with lifestyle + dietary nutraceuticals only.
Curious, quick summary on this?
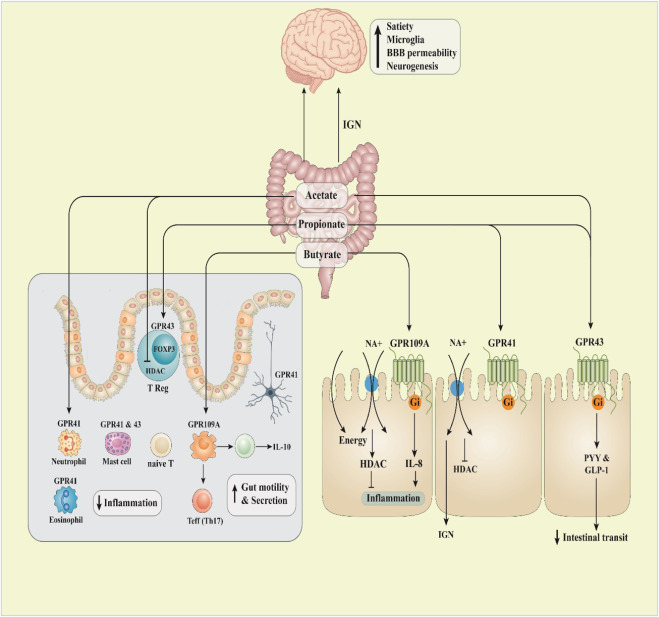
see scfa, typical microbiome expected of older adults vs their microbiome
Identification of gut microbiome signatures associated with longevity provides a
promising modulation target for healthy aging
“In general, gut microbiome diversity decreases during aging…an increase in potentially beneficial bacteria known as short chain fatty acids (SCFA) producers (e.g. Akkermansia, Clostridium). Japanese cohort had greater gut microbiome diversity than the younger group”
The gut microbiome of healthy long‐living people
“Features that differentiate the long-living individuals from the younger group were shared. Again, these features included the greater microbiome diversity and several enriched OTUs (operational taxonomic units) related to SCFA production. We thus hypothesize that modulation of the gut microbiome (e.g., via diet, probiotics) to maintain a healthy gut microbiome will promote healthy aging. One rationale behind this hypothesis is inflammaging, i.e. increased chronic, low-grade inflammation in the elderly, which is associated with different chronic diseases. SCFAs are important in maintaining gut hemostasis. SCFAs provide the primary energy for colon epithelial cells and possess anti-inflammation properties. The enrichment of these SCFA producers in long-living individuals suggests that these bacteria might reduce inflammation and its resulting damage in this cohort, which likely contributed to their healthy aging”
I started adding green banana flour to my meals for exactly this reason, to enhance SCFA, but wasn’t rigorous. Need to re-initiate.
https://goqii.com/blog/green-banana-flour-9-reasons-to-switch-to-this-super-food-today/
A diverse diet is associated with longevity.
Dietary Diversity and Healthy Aging: A Prospective Studyhttps://pubmed.ncbi.nlm.nih.gov/34073820/
“Food consumption may influence the aging process, and adherence to a diverse diet is associated with a healthier aging process in elderly people”
what are the long term implications of acarbose? most of what i read indicated digestive issues that resolve once discontinued
It’s been used for a long time. In fact, acarbose is used over metformin in some countries. If there were any complications in that time frame, we would have probably seen it. But I can’t rule out any additional safety issues - particularly with individuals - I can only speak to my own safety risks. I also try to minimize the meds I use as much as possible that have possible drug-drug interactions. Acarbose isn’t systemic and its possible metabolite(s) has no interactions afaik.
Not only that, there are multiple natural forms of alpha-glucosidase inhibitors like acarbose in the traditional Okinawan diet. That’s what I use on top of occasional acarbose.
Used for more than 100+ healthy years for some centenarians - who’ve naturally inhibited mTOR periodically with calorie restriction and inhibited alpha-glucosidase as well. Probably safe for me but who knows?
I find it weird people are so fixated on metformin when it’s a “dirty drug” with a lot of possible off-targets when acarbose was the one that had decent results for male mice in the gold standard NIH/NIA ITP while TAME failed spectacularly in humans and metformin alone in rats failed.
Perhaps it’s just because it’s more widely used in the US with more press and people love to follow the crowd. I also assume people don’t like acarbose because of harmless gas. But who knows?
I do also follow the metformin research and I have some metformin btw for certain emergent situations but never used it so far. Needs a lot more data for frequent use is my guess.
The most recent ITP trial shows acarbose + rapamycin led to ~30% median lifespan extension in male rats - the best possible result so far in the gold standard so I’m not really sure why it’s worth risking infections with canaglofozin. Btw Re: @David figured you’d be interested in this one.
could you provide some examples of these natural forms? greatly appreciated
The obvious one is Okinawan purple sweet potato the staple - tons of sugar and starch in an ultra-high carb diet with apparently young gut flora mixes and no issues in centenarians? Pretty glaring one for anyone that has studied biochemistry, nutrition, and biology.
It literally doesn’t make sense based on consensus nutritional guidelines…until you break it all down very carefully.
A problem though is - people including researchers aren’t careful and don’t follow exactly what the centenarians actually did. Then we get misinformation on whether it had anything to do with it because different methods can produce different results.
The media also has a role in confusion. I had to literally interview these centenarians in person to figure out what actually is real vs fake. And then carefully check every single step. Unfortunately, the literature was not that helpful beyond indirect help of figuring out the spectrum of possibly drug-like nutraceuticals in the whole diet (as well as any external things - even something as simple as centenarians sharing saliva with young ones) and how these thousands of compounds possibly interact, on top of effects on humans.
I’ll just say just because you use the examples - doesn’t mean it’ll work. As a simplified example to illustrate a direct problem, this purple sweet potato must be heated to a certain amount to avoid disabling the inhibitor because raw would mean there are peroxidases chewing the natural inhibitors up. It requires in-depth biochemical understanding to know where to look and come up with plausible mechanisms that will affect your results. Then you need to test it empirically - not just being an expert in theory. You can’t just copy blindly - otherwise, you’re wasting a huge amount of your money over a lifetime buying these expensive spuds.
Unfortunately, you will find no mention of that in the literature afaik although there are analogous chemical reactions and known peroxidases found in regular sweet potatoes in the literature if you dig it, then check the alpha-glucosidase inhibitor chemical structure of anthocyanins (pretty straightforward if you understand what’s in blueberries) - pretty easy to put it together and realize it’s a real issue. If you run experimentals with purple sweet potatoes sample with the professional lab equipment that I use, you can easily replicate this issue (hopefully a researcher replicates it and publishes it) of not actually translating due to misinformation and blind following.
@tongMD Thank you! I am really interested in Acarbose. I like the idea of using it with starchy meals.
Seriously, I have just one question for those who are currently taking Acbose: Does it make you fart a lot or not?
It does for me - and it’s a good thing - it means it’s working - the bacteria are fermenting the carbs and you’re not getting a huge spike while also getting all those short-chain fatty acids - but I only use it for a very high-carb meal (ie have to deal with some social event where they push say large french fries and a burger)
Want a cheap working (indirect) nootropic? It’s pretty decent frankly when the bacteria are your USP grade supplement factory.
@tong - If you have time, can you give an example of the traditional Okinawa diet that you would eat in a day? I really want to try it!
Btw I would also note that bacteria are really good at adapting, that’s why I use multiple forms so they can’t beat it off - kind of like multiple antibiotics but in this case “naturally occurring in food” under different forms other than acarbose like and mostly nonsystemic.
Lots of microbiology and immunology are involved…but basically you can check to see the spectrum of flora in multiple samples from Okinawan centenarians - it is in the literature as well.
Acarbose bacterial resistance:
I’m still waiting on a future event before I can freely publish my entire library and data on it. I also need to sit down and transfer photos of all my written notes way back with my assistant including cooking instructions, mechanistic rationale and such even after that event.
But basically, my point is - they have a lot of plant-derived compounds from foods (they use “food as medicine” approach) that actually appear to work in very specific conditions, and the Okinawans actually copied the Chinese to a large extent actually when they sent this Okinawan guy to Beijing to learn from the dietary physicians (at the time Chinese physician ranking was “dietary medicine” at the top). It’s in the history books. I have read most of the classical Chinese medical, herbal, and dietary textbooks of that time period so a lot of the “diet as medicine” reasoning Okinawans were doing made more sense.
I found it weird that Western observers have always taken interest in acupuncture and TCM disease classification systems here in the US but not much written about Chinese “dietary medicine” in terms of TCM. Maybe it’s just because nutrition is pretty much at the bottom of prestige here in the US for physicians - kind of the opposite. And of course, nutrition is highly complex with multiple controversies and difficult to study beyond say NHANES data. Nearly nobody wants to fund a 10-20+ years trial.
Traditional Chinese medicine has a few gems to offer too, although I don’t practice any of it and I rarely if ever think of a reason to refer a patient to a US TCM provider. (I’m not a particular fan of almost all herbal extract supplements either) The most obvious one is the malaria drug artemisinin. But unfortunately, a lot of work on actual scientific mechanisms for a lot of parts is needed before a lot of these gems can be extensively proven in human trials. At least they already passed a decent 100+ year “trial”.
Look forward to seeing when it comes out. I was just curious what a typical breakfast, lunch and or dinner would look like. The Chinese connection is interesting!