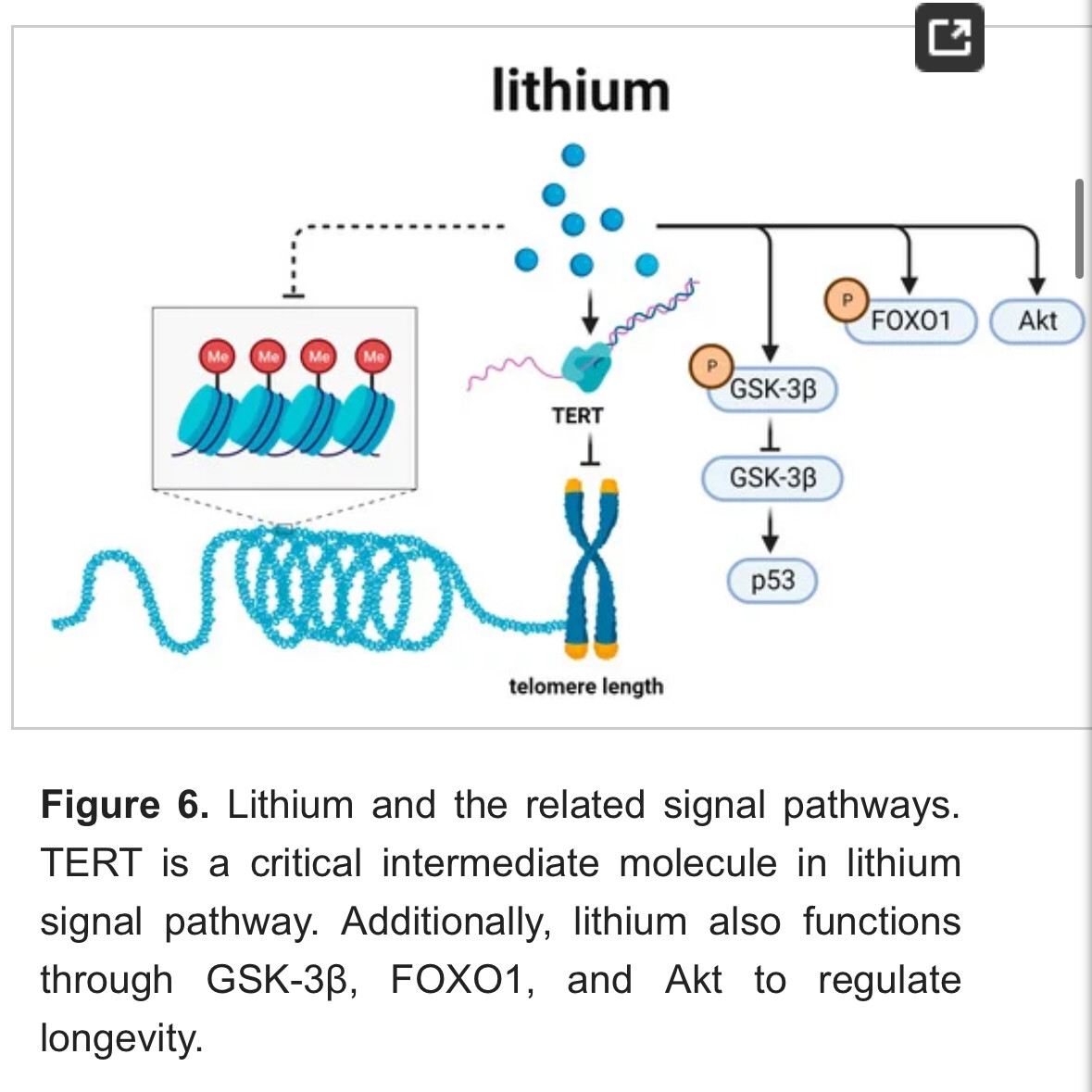
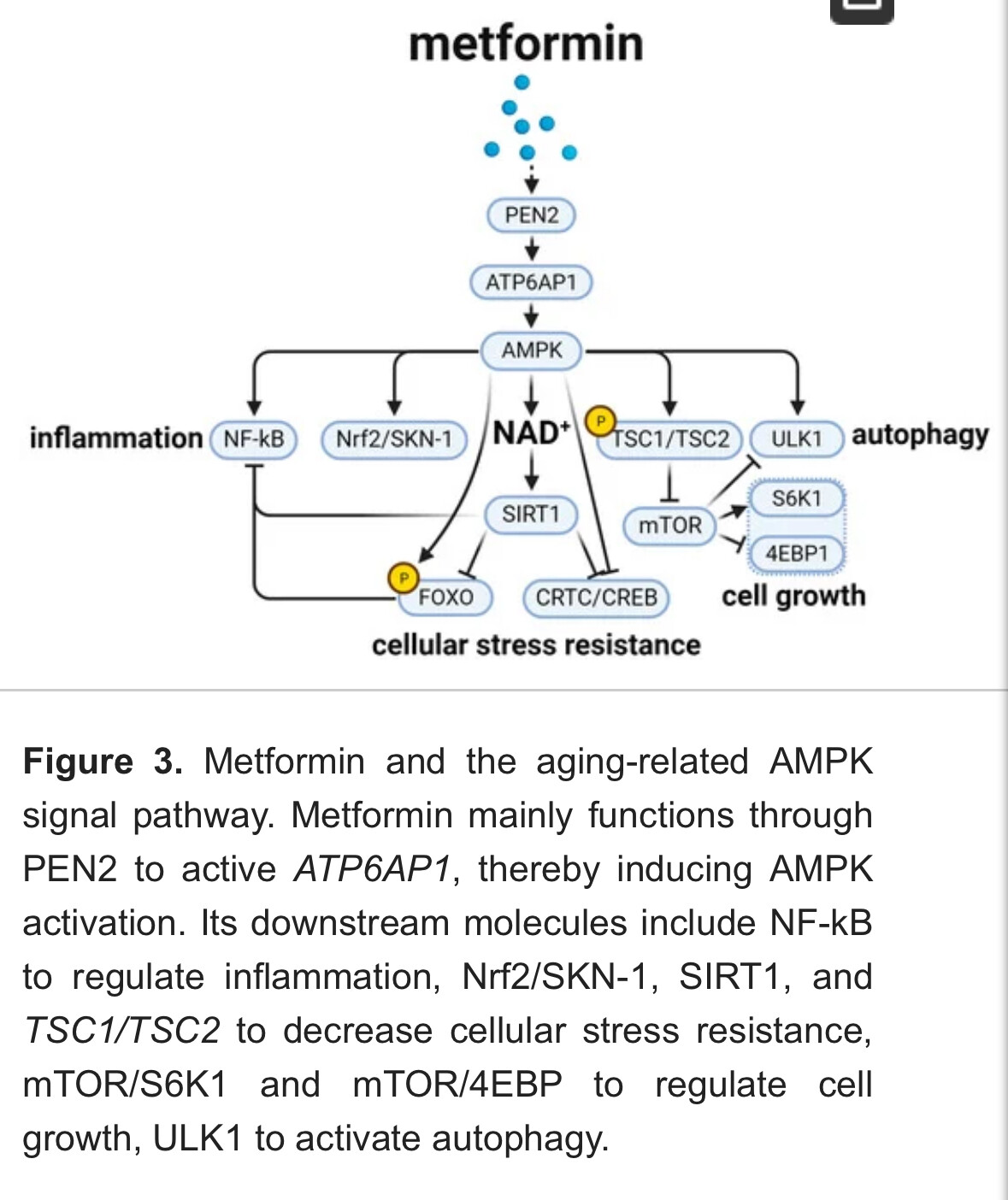
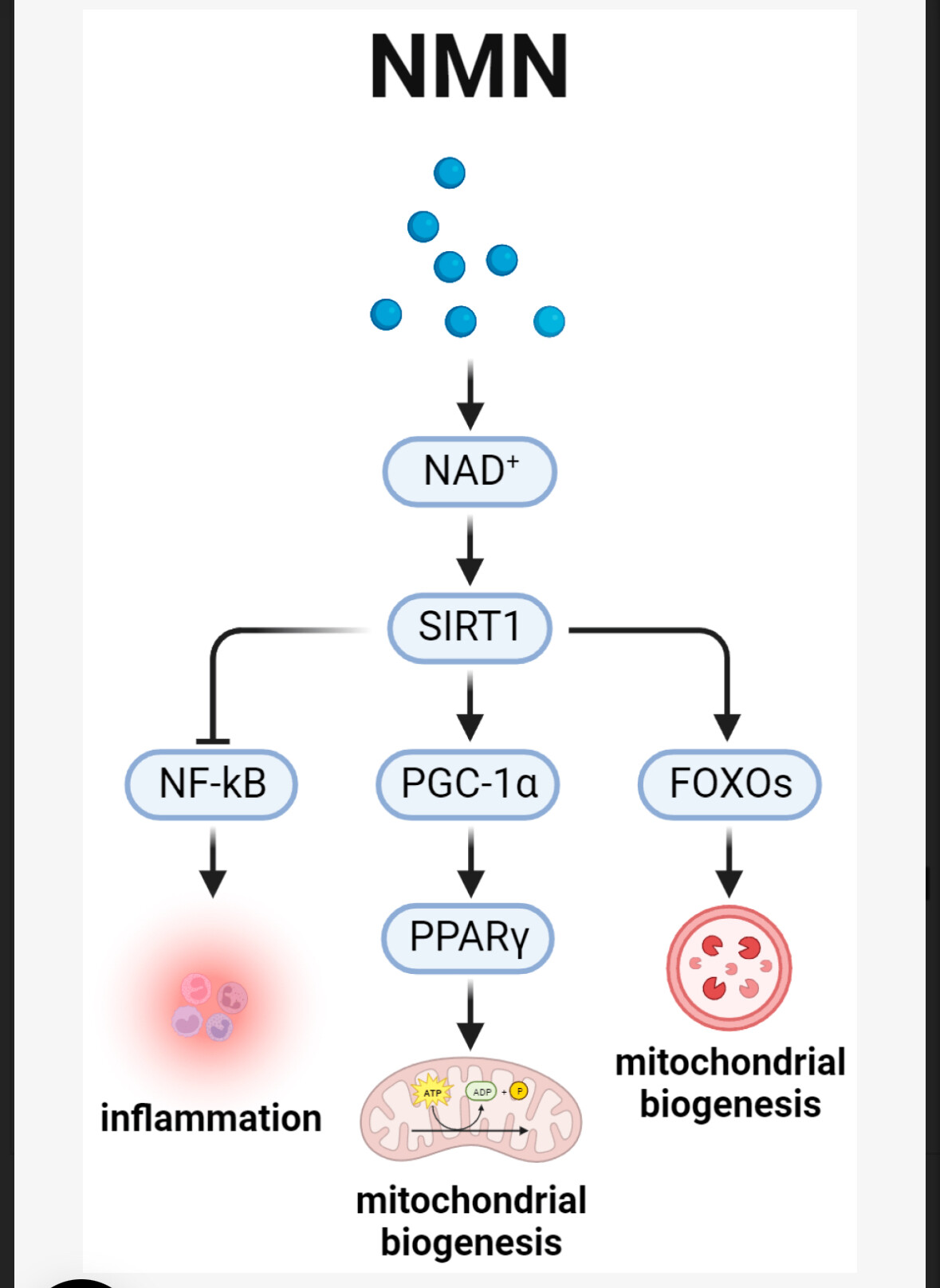
A fairly concise review of six anti-aging pathways and the drugs which affect them, including acarbose, lithium, metformin, NAD+, NSAIDs, metformin and rapamycin.
Aging is a multifactorial biological process involving chronic diseases that manifest from the molecular level to the systemic level. From its inception to 31 May 2022, this study searched the PubMed, Web of Science, EBSCO, and Cochrane library databases to identify relevant research from 15,983 articles. Multiple approaches have been employed to combat aging, such as dietary restriction (DR), exercise, exchanging circulating factors, gene therapy, and anti-aging drugs. Among them, anti-aging drugs are advantageous in their ease of adherence and wide prevalence. Despite a shared functional output of aging alleviation, the current anti-aging drugs target different signal pathways that frequently cross-talk with each other. At present, six important signal pathways were identified as being critical in the aging process, including pathways for the mechanistic target of rapamycin (mTOR), AMP-activated protein kinase (AMPK), nutrient signal pathway, silent information regulator factor 2-related enzyme 1 (SIRT1), regulation of telomere length and glycogen synthase kinase-3 (GSK-3), and energy metabolism. These signal pathways could be targeted by many anti-aging drugs, with the corresponding representatives of rapamycin, metformin, acarbose, nicotinamide adenine dinucleotide (NAD+), lithium, and nonsteroidal anti-inflammatory drugs (NSAIDs), respectively. This review summarized these important aging-related signal pathways and their representative targeting drugs in attempts to obtain insights into and promote the development of mechanism-based anti-aging strategies.
Full paper, Open Access: Biomedicines | Free Full-Text | Anti-Aging Drugs and the Related Signal Pathways
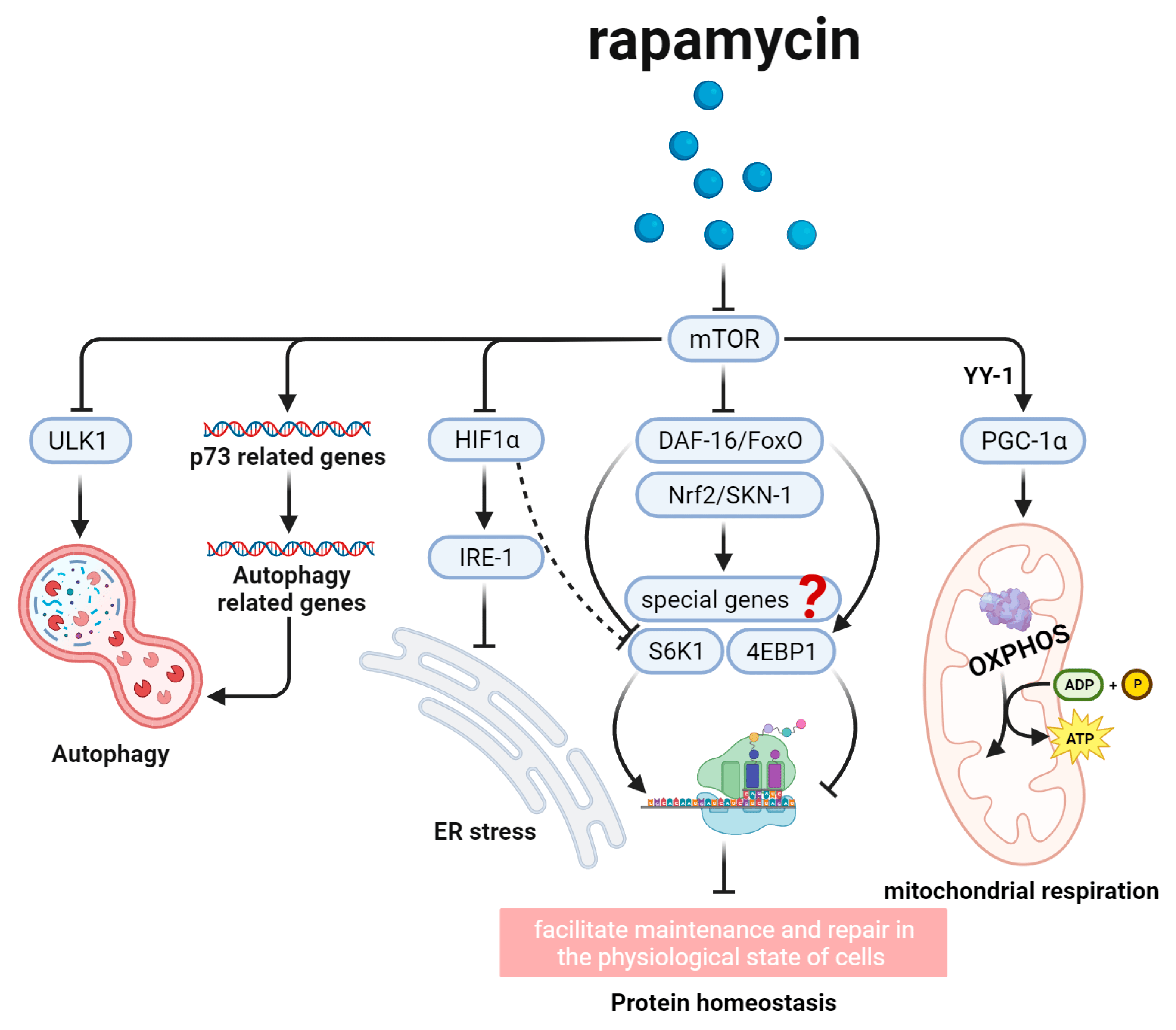
Figure 2. Rapamycin and the aging-related mTOR signal pathway. This figure shows several signal pathways downstream of rapamycin. Rapamycin mainly functions through mTOR and their downstream molecules, such as DAF-16/FoxO and Nrf2/SKN-1, to regulate protein homeostasis, PGC-1α to influence mitochondrial respiration, ULK1 and p73to regulate autophagy, and HIF1α to inhibit ER stress, aiming to regulate longevity.
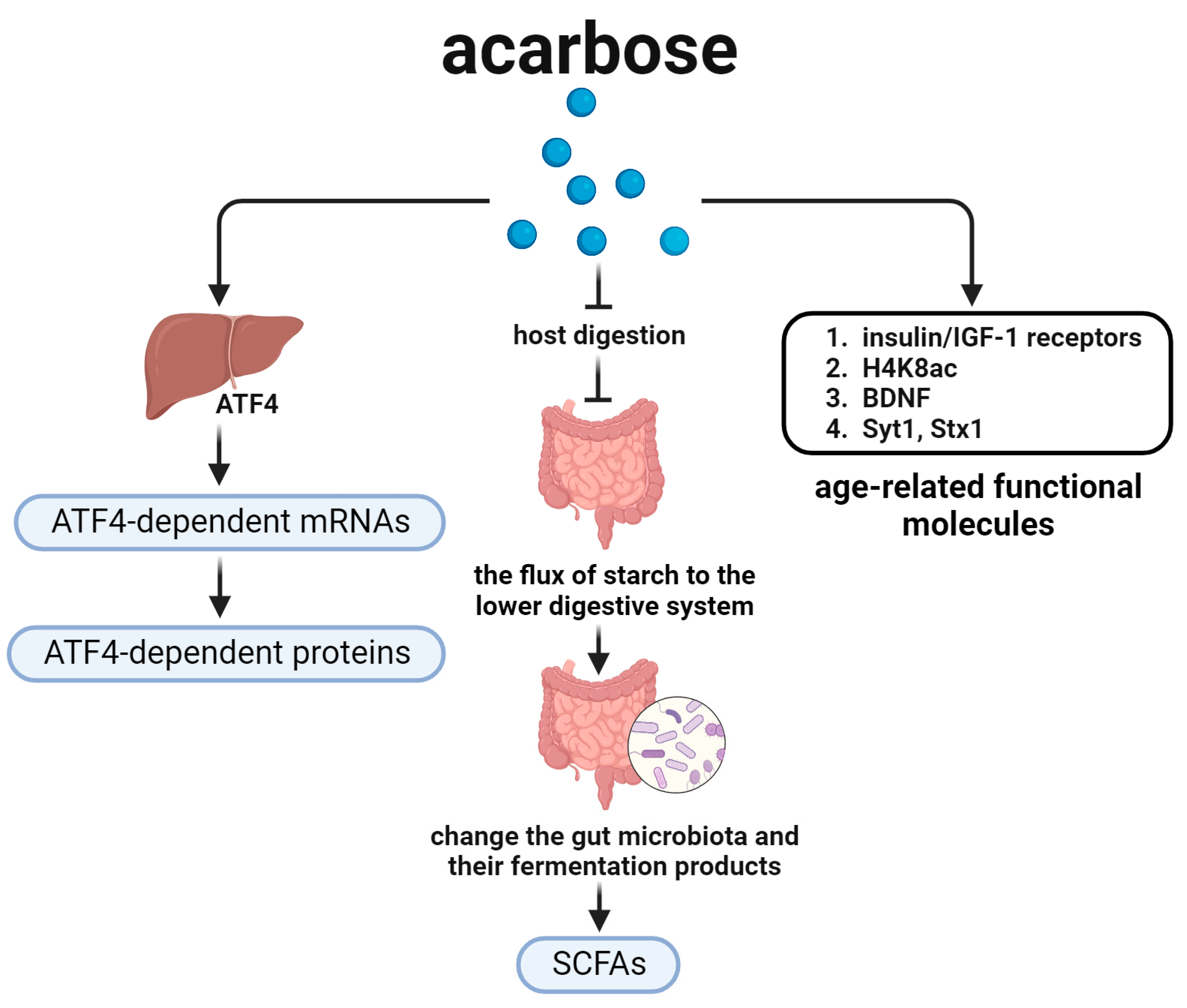
Figure 4. Acarbose and the aging-related nutrient signal pathways. This figure shows several signal pathways downstream of acarbose. Acarbose may change the gut microbiota, insulin/IGF-1 receptors, and ATF4 to regulate lifespan.