Okay, okay! I won’t switch from telmisartan. ![]()
1 Like
Haha it’s okay. I just didn’t want people reading us to believe that ACEI/ramipril was significantly better than ARB/telmisartan for stroke prevention as current evidence doesn’t show this. Of course, future studies might change the conclusion. But as of today, the best first line anti hypertensive seems to be a combination [telmisartan + (amlodipine and/or indapamide)].
2 Likes
Just to be clear, is there an intrinsic reason why telmisartan + amlodipine and/or indapamide are superior to higher-dose telmisartan, or is it simply the aversion of possible side effects that come from higher-dose telmisartan? In other words, if a patient is effectively controlling hypertension with 80 mg telmisartan without side effects, is it nonetheless beneficial to switch to lower-dose telmisartan + amlodipine and/or indapamide?
I mentioned the two-drug combination for therapy initiation only. Here’s the rationale: Optimal Blood Pressure we Should Target? Systolic Under 110 or 100? - #244 by adssx
If someone is already on telmisartan 80 mg monotherapy and well-controlled: If it ain’t broke, don’t fix it? ![]()
5 Likes
Preprint but great team: Association between Class of Antihypertensive Drugs and Risk of Incident Dementia: A Multinational Population-Based Cohort Study 2024
1,982,839 individuals followed over more than 6 years in 4 countries (UK, HK, Sweden, and Australia):
Our study supports the use of ARBs compared to ACEI when considering the risk of cognitive decline and dementia, based on a multi-ethnic cohort with a long median follow-up time.
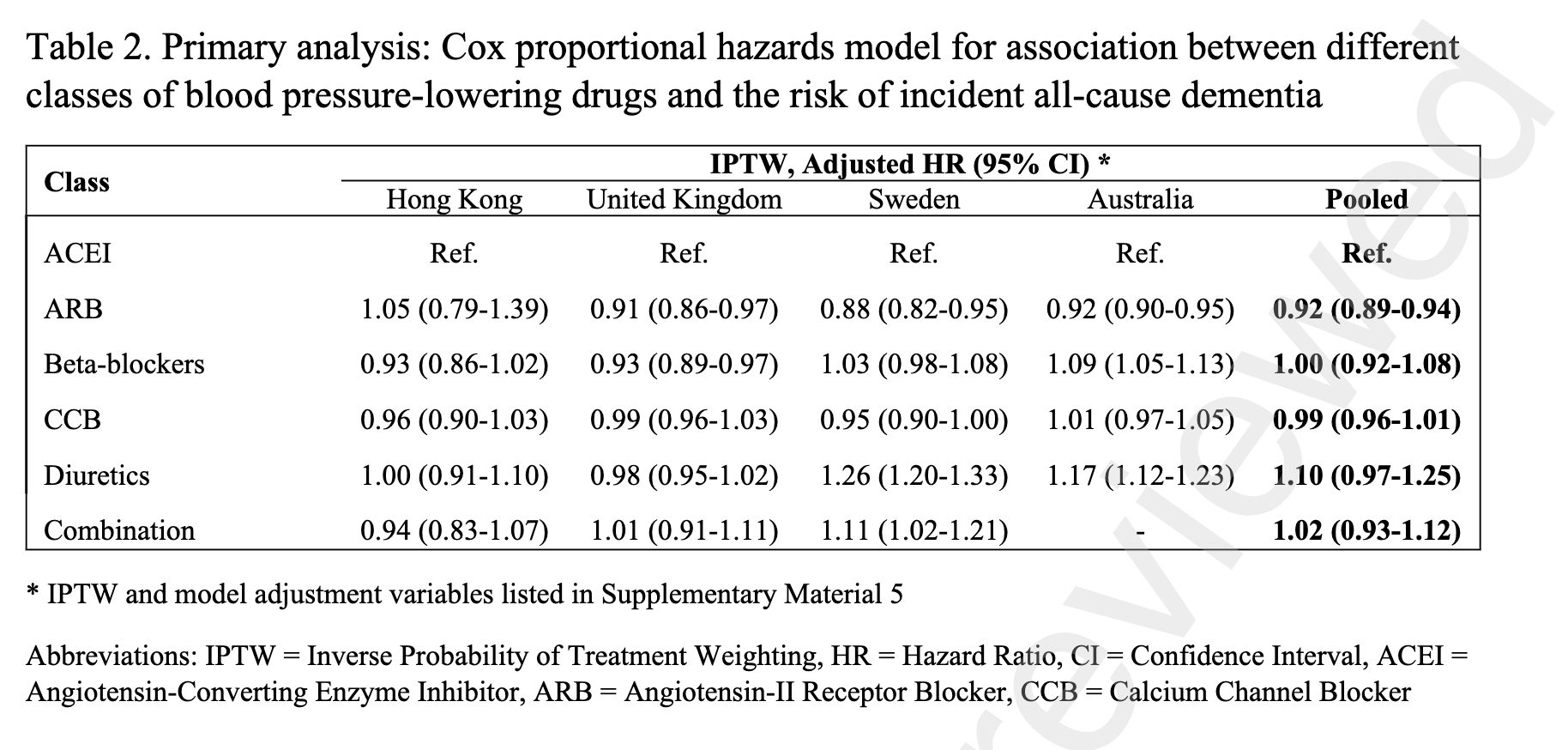
Unfortunately, they didn’t do the job properly and didn’t distinguish DHP CCBs (e.g., amlodipine, associated in many studies with lower rate of dementia) from non-DHP CCBs and thiazide/thiazide-like diuretics (e.g., indapamide) from other diuretics (e.g., loop diuretics).
2 Likes
What is the lowest effective dose of Telmisartan? I saw you guys mentioned 20 mg, but my pharmacy only gives 40 mg. Is 20 mg still highly effective? @adssx @desertshores
I broke 40 milligrams of telmisartan into two parts, so half a tablet is 20 milligrams per day
1 Like
Thank you. I just did a search and it confirms you can split it in half with no lose of efficacy
2 Likes
You can split pills, but off-target benefits of telmisartan seem to appear above 40 mg per day (for insulin resistance) and 80 mg per day (for PPAR-alpha inhibition).
5 Likes
@DrFraser
Thanks for the post. In another post, you mention you like to increase telmisartan up to 80 mg for its effects on ppar. Can you elaborate on your decision tree whether to go to 40 vs 80 mg in any given individual? Thx.
2 Likes
In general, so long as there is no contraindication (e.g. they are having some renal dysfunction, hyperkalemia, hypotension) with lower dose telmisartan, I’m pushing to 80 mg on this, as most individuals are interested in neuroprotection. There is some literature stating the effect probably is still not that potent at 80 mg, and potentially going to 160 mg. I’ve not done that yet.
It really is an issue of tolerability and lack of contraindication - and if those conditions are met, 80 mg is my approach before adding a second agent for hypertension.
There are lots of factors that might push me in individual cases to choose something different first, if they had a specific other condition favoring another compound, but patients with normal labs, and enough BP to tolerate this medication, will usually have it recommended by me, for neuroprotection and hypertension (as defined by SBP>120 not SBP>130-140 mmHg).
Hopefully that answers the question?
8 Likes
Yes, thank you. Very helpful.
Would we have to worry about any nutrient deficiencies from going with an 80mg or higher dose of Telmisartan?
At the 80 mg dose, I don’t think it is potent enough to have me head down that rabbit hole. It would be unclear to me with stronger PPAR effects as to whether any situation beyond a diverse diet, mostly plants, appropriate fiber would have any evidence.
I was looking through this recently - and as much as it modulates a lot of things, I don’t really see anything I’d recommend on diet beyond my usual advice.
I’d love if you or someone else had some evidence on this or concerns as it is a good question, and one I’ve not worried about at the 80 mg - but perhaps at 160 mg, it might be an issue to contemplate at least.
2 Likes
The results suggest the use of ARBs such as candesartan in PD patients, particularly before and after dopaminergic grafts, and the need to monitor AT1-AA levels in PD patients, particularly in those candidates for dopaminergic grafting.
1 Like
I’m tolerating the 80mg dose of telmisartan well, with the only side effect being a mild headache at night, but not enough to significantly interfere w/sleep.
The hard part has been trying to get off my beta-blocker (nebivolol). Everything is good while at 5mg (a pretty low dose), but even slowly weaning down to 2.5mg for a week and then stopping after another week caused significant tachycardia, albeit normal blood pressure. Back to 5mg now, and everything is great. It would be great to completely come off, but it might require an even slower taper.
Why do you want to come off nebivolol? If you have tachycardia, it’s a great treatment, isn’t it? Alternatively, you could use carvedilol?
1 Like
I only got tachycardia as a result of coming off the beta-blocker, since the medication lowers heart rate and my heart has become accustomed to being on nebivolol for so many years. It’s likely just going to require a significantly longer time to taper off.
1 Like
Starting to read up on this a bit - has anyone come across good MR studies?
@adssx do you think that the effects are independent of blood pressure or are the effects from getting people closer towards optimal blood pressure?
i.e. while these effects are increasingly looking promising for people with average (or bad) blood pressure do you think they would be there also for someone with optimal blood pressure too?
I just had to discontinue Nebivolol. I was getting all the hypothyroid symptoms from it and I read a study showing certain beta blockers reduced T4 to T3 conversion so it’s possible the same effect happens with Nebivolol. My thyroid conversion was already poor enough.
1 Like