Thanks
Still, another cheap intervention to try.
It has higher customer ratings on Amazon, not that it means anything, but most enjoy the tea.
It looks like there are studies to back up the benefits claims. Pub Med has many articles establishing its benefits
"Various review articles have highlighted other potential benefits of hibiscus tea, including:
Several studies have demonstrated the potential of hibiscus tea in lowering blood pressure:
A randomized controlled trial ([2]) found that consuming hibiscus tea for 6 weeks significantly reduced systolic blood pressure (SBP) by 7.2 mmHg compared to placebo in pre- and mildly hypertensive adults.
A systematic review and meta-analysis ([3]) showed a significant reduction in both systolic and diastolic blood pressure with hibiscus supplementation, with greater effects observed in individuals with higher baseline blood pressure levels.
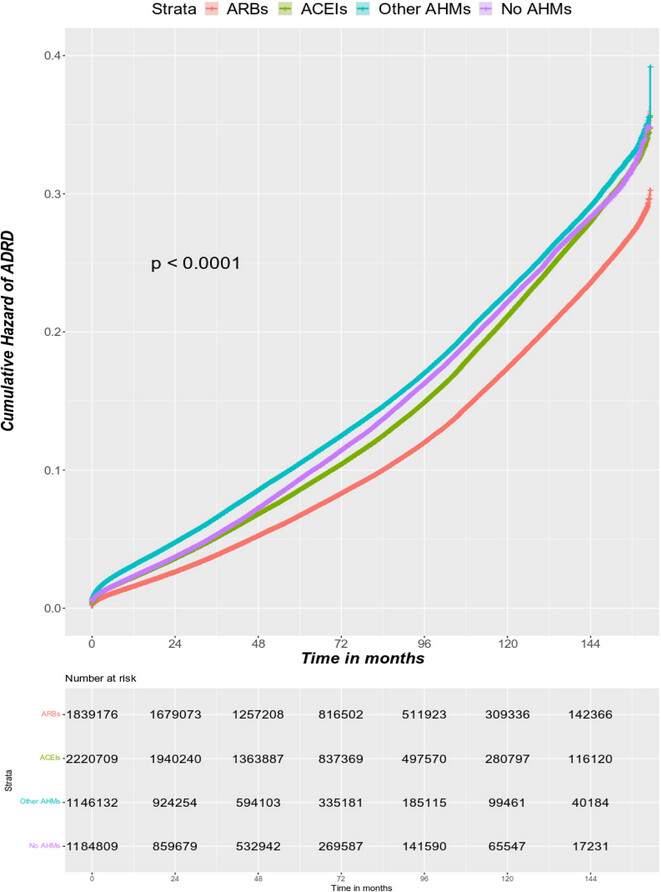
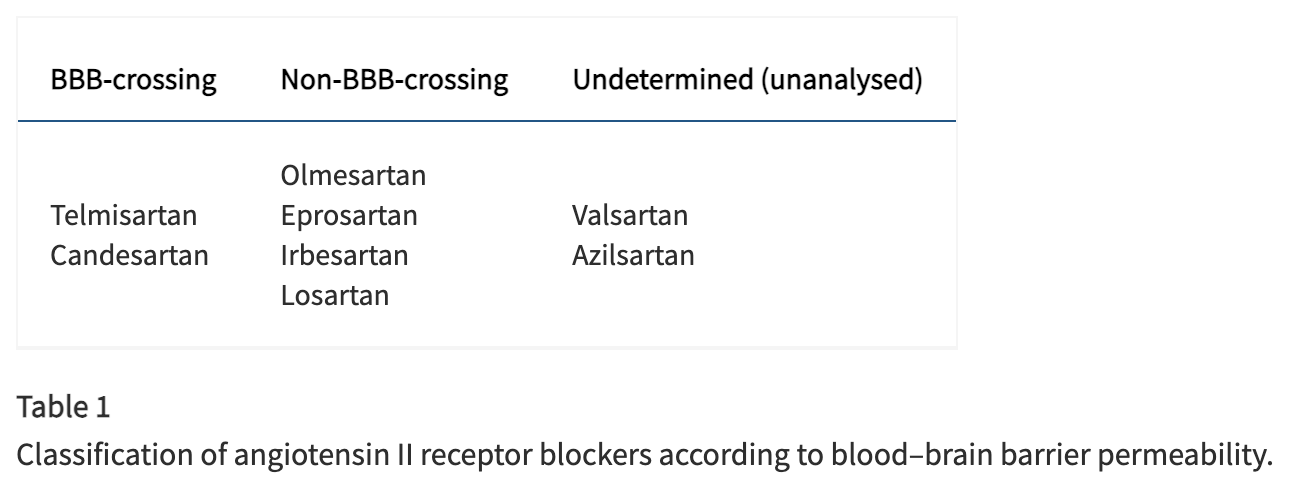
Neuroprotective effects and potential benefits in Alzheimer’s disease ([1])
Nephroprotective, antianemic, antioxidant, anti-inflammatory, and anti-xerostomic activities ([5])
Potential therapeutic applications in cancer and inflammatory diseases ([6])
Antimicrobial and antioxidant activities
Several studies have suggested that hibiscus tea may have beneficial effects on lipid profiles:
A review article ([4]) indicated that hibiscus extracts can improve lipid profiles by reducing total cholesterol, LDL cholesterol, and triglycerides.
A review article ([5]) highlighted the antidyslipidemic effects of hibiscus preparations reported in clinical trials.