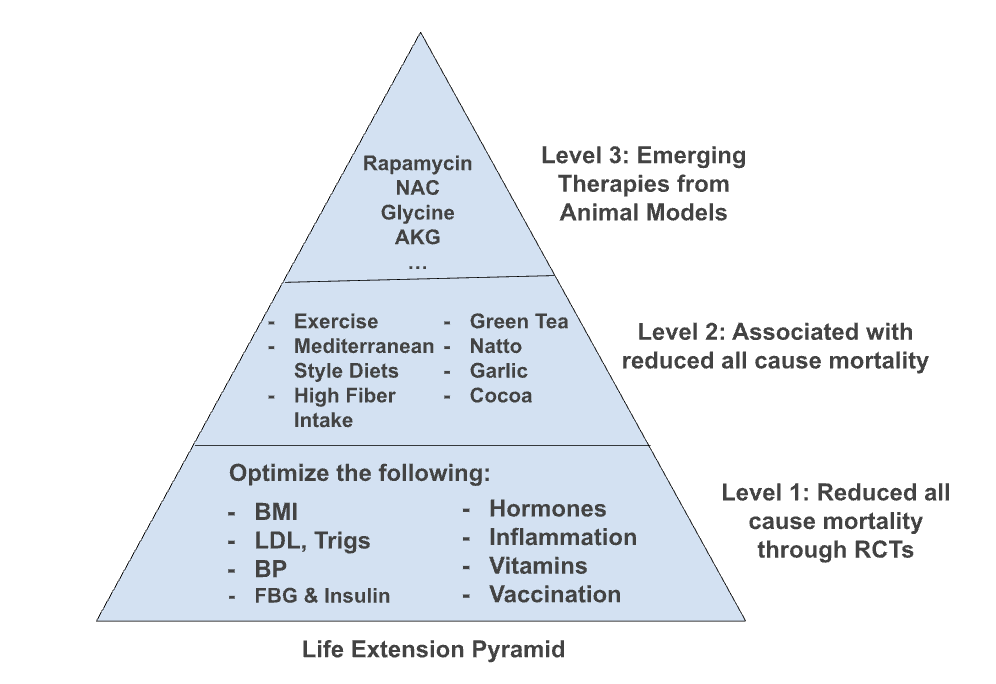
This post outlines a practical, three-tiered framework for prioritizing longevity interventions based on the strength of scientific evidence.
Tier 1: Highest Evidence (Proven in Human Trials) The foundation of any longevity strategy should be interventions proven to extend lifespan or reduce all-cause mortality in human randomized controlled trials. These include:
- Sustained weight loss, achieved through lifestyle changes or, when necessary, medication.
- Cardiovascular risk reduction through LDL cholesterol lowering (especially with statins) and intensive blood-pressure control.
- Comprehensive prevention via “polypill” strategies.
- Testosterone replacement therapy (TRT) for men with clinically low levels. An equivalent strategy for women.
- Annual flu vaccination.
- Modest benefits from supplementation with multivitamins, vitamin D, and EPA-rich fish oil.
Tier 2: Strong Associational & Preclinical Evidence This tier includes practices with strong positive associations in human observational studies and/or proven lifespan benefits in animal models.
- Lifestyle: Regular exercise, a Mediterranean-style diet, and social well-being.
- Diet & Supplements: Coffee, green tea (EGCG), cocoa, garlic, fiber, glucosamine, and natto (for spermidine and vitamin K2).
- Pharmaceuticals: Aspirin (data remains mixed).
Tier 3: Emerging & Experimental Interventions These options have shown promise in animal models and have preliminary signals in human studies but require more research. They represent the cutting edge of longevity science.
- Dietary Strategies: Calorie restriction, one-meal-a-day (OMAD), ketogenic, or lower-carbohydrate diets.
- Pharmaceuticals & Supplements: Rapamycin, metformin, acarbose, canagliflozin, pioglitazone, taurine, spermidine, creatine, glycine, glycine+NAC, AKG, astaxanthin, curcumin, resveratrol, grape-seed extract, vitamin C, icariin, Glylo, and Protandim.
- Controversial: NAD+ boosters and fisetin.
Guiding Principles Regardless of the tier, always work with a physician to guide your choices and treat any abnormal biomarkers. Track your personal responses (N=1 analysis), and remember that interventions improving quality of life can be valuable even without proven lifespan benefits. De-prioritize interventions based solely on mechanistic theories until stronger evidence is available.