Yes - good questions. I’m not sure of the answers - I was just posting one doctor’s opinions.
I usually take my empagliflozin just like you - an hour before any meal, in the morning (but typically just eat lunch and dinner). I think you want the peak, or higher blood levels during the time of the day you’re eating your main meals… but I’m not sure what the effect would be if I took it at night. Something to test when I have my CGM on - to see the difference.
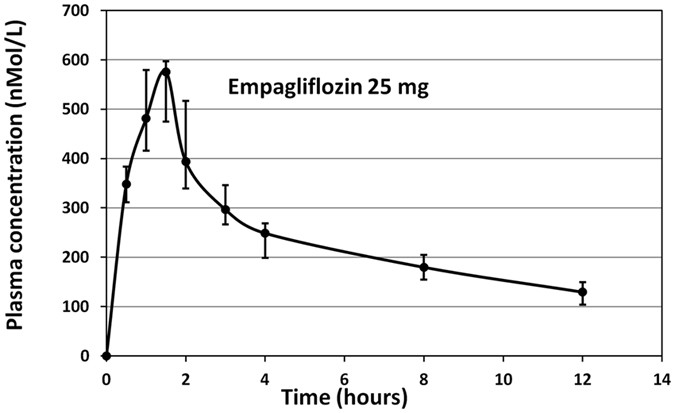
Here is the blood level curve below:
Yes - the SGLT2i drugs lower peak blood glucose levels. After reading that doctor’s comments I’m going to try at some point dosing at night and seeing what impact it has on fasting blood glucose levels in the morning. An interesting experiment.
I’d be very interested to see your results! For the usecase of consuming at night , I also wonder if metformin/berberine would be a better option (ignoring effects on exercise here, or assuming one’s being sedentary around the days of ingestion). Metformin would be explicitly reducing the amount of gluconeogenesis but sglt2i will only prevent reabsorption of any high levels of sugar in the kidney.
I don’t calibrate my acarbose dose with my rapamycin dose, in any way at all. I treat it completely separate. I started with 25mg of acarbose with every meal and slowly increased it (if you’re new to acarbose and if you have a diet with significant amounts of wheat-based products, you’lll find the gas/flatulence can be a little overwhelming). As I’ve moved my diet mostly away from wheat based products (towards more rice, lentils, etc.) the flatulence issue has largely resolved and I typically take 100mg with every meal. Some people here take upwards of 200mg with every meal.
We (as a community here) haven’t put nearly as much thought and effort into the acarbose dosing question as we have for the rapamycin dosing question. It is something we should perhaps investigate more and test more.
Given the research showing no statistically significant impact on HbA1c between 50mg and 200mg with food, I would argue that taking just 50mg with carb-dense food is sufficient and very affordable.
It depends what you think the method of action is, for the Acarbose driven life extension. if you think its just the blood glucose levels & spikes, then you are correct. If you think its potentially other mechanisms, then perhaps you want to try higher dosing.
In the ITP studies they dosed between 400ppm, 1000ppm and 2500ppm compared to dosing between 14ppm and 44ppm for rapamycin (ppm in the food).
For Acarbose:
The two higher doses produced 16% or 17% increases in median longevity of males, but only 4% or 5% increases in females. Age at the 90th percentile was increased significantly (8%–11%) in males at each dose, but was significantly increased (3%) in females only at 1,000 ppm.
The lowest dose of ACA did not change median survival (0% increase), but significantly (p = 0.03) improved survival at ages greater than the median (Table (Table1,1, Figure Figure1a).1a). ACA had much more benefit in males, whose median lifespans were increased by the three doses by 11%, 17%, and 16%, respectively, all highly (p < 0.0001) significant (Table (Table1,1, Figure Figure1b).1b).
Have you done the math on the dosing from 400ppm to 2500ppm? (for a 50kg to 70 kg person) (I haven’t - thats why I’m asking). A quick glance seems to suggest that 400ppm equates to about 350mg for a 70kg person.
If someone wants to do it, they could use this Dramamine model that we used earlier:
My calculation shows that the ITP fed the mice a human equivalent dose of about 730mg of Dramamine per day for a 70kg person.
Here is the math:
The ITP used 800ppm in food (see attached photo). And 800ppm is 0.08%. A typical mouse weighs about 0.025kg and eats about 4g of food per day, so 0.08% is 3.2mg of Dramamine for the mouse per day. That is a dose of 3.2mg/0.025kg=128mg/kg. Divide by 12.3 to allometrically scale to humans, to get a human equivalent dose of (128mg/kg)/12.3=10.4mg/kg. So for a 70kg human, that would be 728mg of Dramamine per day.
OK, please check my math. If this Math is correct (and you could get Acarbose very cheaply) how much would you take, and why?
The ITP did not find any acarbose (ACA) longevity benefit (in terms of median survival) in the 400ppm for the combined pool or females and males, only the 1000 and 2500ppm dosing. However, ACA had much more benefit in males, whose median lifespans were increased by the three doses by 11%, 17%, and 16%, respectively, all highly (p < 0.0001) significant
The ITP has in a series of studies (See Acarbose Details) done Acarbose dosing at 400ppm, 1000ppm and 2500ppm (starting at different ages).
The ITP used 400ppm in food. And 800ppm is 0.04%. A typical mouse weighs about 0.025kg and eats about 4g of food per day, so 0.04% is 1.6mg of Acarbose for the mouse per day. That is a dose of 1.6mg/0.025kg=64mg/kg. Divide by 12.3 to allometrically scale to humans, to get a human equivalent dose of (64mg/kg)/12.3=5.2mg/kg. So for a 70kg human, that would be 364mg of Acarbose per day. Assuming it split evenly between 3 meals a day, thats about 120mg/meal.
1000ppm
This is 2.5 times the dose of 400ppm, so multiply by 2.5.
Total Acarbose per day: 910 mg. Assuming it split evenly between 3 meals a day, thats about 300 mg/meal.
2500ppm
This is 2.5 times the dose of 1000ppm, so multiply again by 2.5.
Total Acarbose per day: 2275 mg. Assuming it split evenly between 3 meals a day, thats about 860 mg/meal.
True, but there is still a dose response. We just don’t know why…
But - it does seem like the benefit maxes out around the 1000ppm, so perhaps thats the ideal intestinal concentration for this drug. There is no added benefit at 2500ppm over the 1000ppm.
more benefit in males, whose median lifespans were increased by the three doses by 11%, 17%, and 16%,
Am I the only one that thinks this is a bit odd. SGLT2’s work in the kidneys which have decreased activity at night. An SGLT2 isn’t going to deplete body glucose, and I don’t know what it means to declutter a mitochondria?
For an average person, taking a SGLT2 inhibitor at night would have an addictive effect on natural circadian rhythm and functions- that’s the hypothesis anyway.
SGLT2 will not “deplete” glucose but yes, the drug will perform functions regulate glucose over night. I can’t think of why it wouldn’t, but regardless it’s proven to do so- day or night.
Results: T max increased by 35% in the evening phase compared to the morning phase, while C maxdecreased by -6.5% in the evening dose compared to the morning dose. Additionally, AUC 0 to ∞increased in the evening phase by 8.25% compared to the morning phase. The mean cumulative amount of glucose excreted (UGE ( 0-24)) increased by 43% in the evening dose compared to the morning dose
Conclusion: Despite the difference in pharmacokinetics parameters between evening and morning doses, C max, AUC 0-t, AUC 0-∞, didn’t differ on the bioequivalence level. In addition, as UGE ( 0-24) didn’t statistically differ, thus, we can conclude that there is no statistical significance between the morning and evening doses.
Biologically speaking, their cannot be a meaningful difference. I don’t mean this personally, but if you do not have a background in molecular biology this can all be difficult to understand, but this website has a group of people with these backgrounds- myself inc. that you can learn from. I have learned so much, we’re lucky to have such a strong forum.