Hopefully this week, I’m going to extract the 17-alpha estradiol from the Pantostin. Isopropanol (IPA) and water (two ingredients found in Pantostin) form an azeotropic point, which is difficult to separate using conventional distillation method.
I’m going to use a process called ‘salting out’ where you add a salt to the homogeneous solution, shake, leave it to stand and the water and IPA separates out into two layers. I’ve got two small measuring cylinders and plan to try two salts, potassium carbonate and dipotassium hydrogen phosphate, head-to-head. I think the phosphate salt may be superior in its ability to separate the water from the IPA.
Two hours later - Wow, I was wrong. Seems like carbonate is the way to go, phosphate was hygroscopic and a pain to weight out. Potassium carbonate also salted out a much larger aqueous layer 6.5 mls compared to 3.5mls after compensating for addition of 2g of salt.
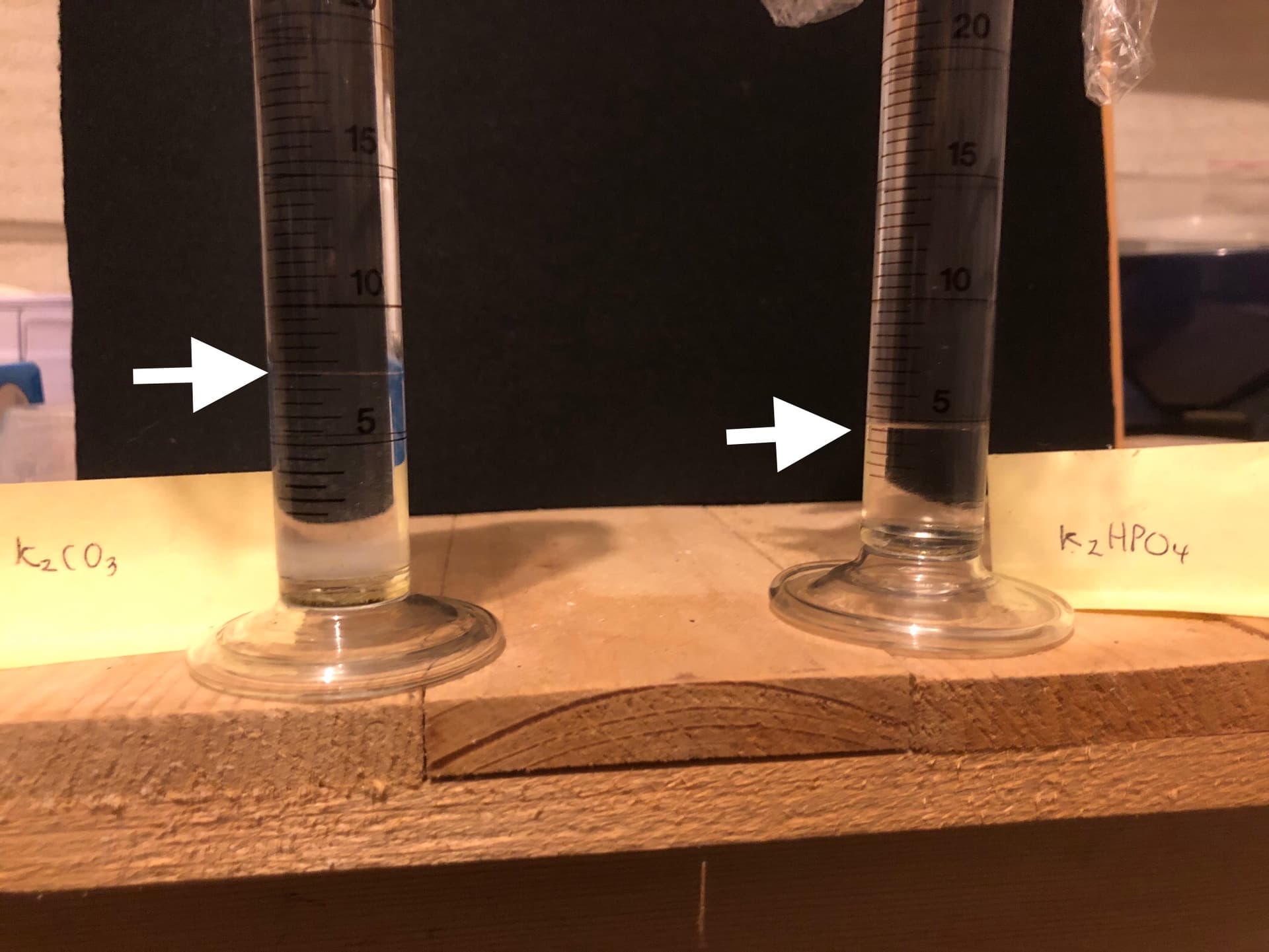
Sorry about the quality of the photos it’s very hard to photograph the meniscus. ![]()
According to the manufacturer Pantostin, as well as containing IPA and water also contains glycerol and inositol both of which are water soluble and of course 17-alpha estradiol which is water insoluble. So when you ‘salt out’ Pantostin you get an upper layer of IPA which contains 17-alpha estradiol and a lower aqueous layer containing inositol and glycerol.
For the record it seems like Pantostin contains 74% IPA.
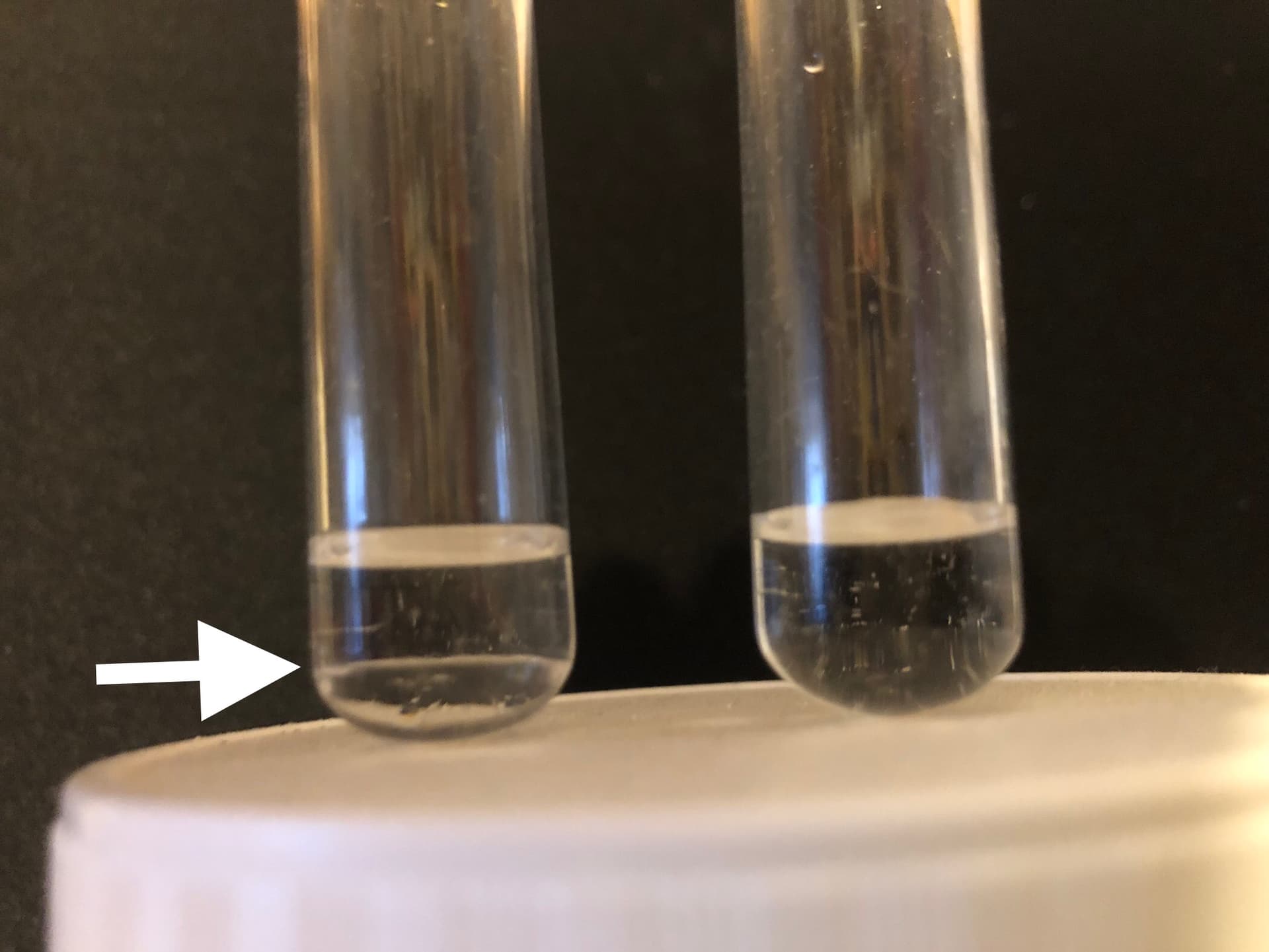
Just to make sure about glycerol I made up two test tubes with glycerol + IPA (left) and glycerol + H2O (right) as you can se below glycerol is immiscible in IPA but soluble in water.
I’m going to leave it overnight, to settle out completely and decant off the organic phase. I’ll then see about doing a second IPA extraction of aqueous layer.
I’m still ‘playing around’ to get an optimal extraction protocol and will post it when I’m happy with it ![]()