If you start with a level that is at the lower end for men, it might be useful to start with the sensitive test to get an accurate baseline. In my case I already know from my last regular Estradiol test that I am at the high end (for men) already, probably due to all my belly fat!
The main goal is to measure the increase in Estradiol level due to the 17-Alpha Estradiol (assuming the tests cannot distinguish it from 17-beta Estradiol). If those elavated Estradiol levels are not in the range normally achieved by HRT in women, that means you are not getting enough 17-alpha Estradiol to get even the same neural benefits that women get from HRT. The mice studies had male 17-alpha Estradiol levels way higher than the 17-beta Estradiol levels in female mice.
My wife gets 50ug of 17-beta Estradiol per day with her HRT (via a patch with 1mg of 17-beta Estradiol per day and an estimated 5% absorption rate). Creams are typically estimated to have a 10% dermal absorption rate for Estradiol, so 1ml of Pantostin (with 0.25ml of transcutol) should result in 25ug of 17-alpha Estradiol per day, so I am hoping the blood test will show a rise to around half the level of the normal HRT target in women. I plan to titrate up slowly up to 4x that level, which gets to the highest level used in HRT for women (100ug/day, corresponding to 4ml of Pantostin per day), unless I observe any adverse effects, or blood tests showing excessive suppression of DHT. Any more feels too risky to me.
Aren’t people taking as much as 1mg orally? Did you get your Pantostin? It seems like it’ll be difficult to measure out 1-4ml with this fancy applicator attachment
My Pantostin also arrived from Germany 10 days after ordering (5 of those days stuck in JFK, presumably the customs warehouse) and I am waiting to take my pre LEF bloood tests next Friday before starting.
The applicator will dispense exactly 3ml (to apply to your scalp). That may work if you need that exact dosage and like the side benefit of hair growth (from the roughly 90% that won’t be absorbed, even with transcutol added). You might be able to mark the levels in the applicator at 1ml or 2ml to apply smaller amounts.
Instead, I will use a dropper bottle and mix 40ml of Pantostin with 10ml transcutol and apply 1.25ml (around 1/2 dropper full) on my skin to get 0.25mg of 17alpha-estradiol with an expected absorption of 25ug (10%). When I increase the dose I will apply it multiple times each day, to make the blood level more uniform. With HRT the best results are from patches that produce 24-hour uniform absorption.
Oral 1mg if taken under the tongue, should be around the same as 4ml of Pantostin + 1ml transcutol on the skin and should have the same 10% absorption rate. Estradiol typically does not absorb well via the intestinal tract, since the liver will break down most of it, based on HRT studies with women.
Oh, you meant just a fake increase in Estradiol and it being a test for 17-Alpha-Estradiol. I’m not so sure that it can’t differentiate between 17-A-E and 17-B-E, maybe 70% that it can’t. Testing sensitive estradiol keeps a check on true estradiol levels, for side effects. So testing both might be preferable. The person in that video earlier tested high on the inaccurate estradiol test, but low on the accurate one.
Interesting… I had not really thought about this… I was assuming that the test could distinguish between the two.
My goal with testing for “estradiol” (which is a common term that really refers to 17-beta estradiol) was actually the opposite… One of the biggest concerns I have about 17-alpha estradiol is that because its a chiral molecule and both the 17 alpha and 17 beta versions are both typically manufactured together, and then separated (to varying levels of success)… I was thinking that getting your estradiol is a way to test to make sure you’re getting mostly the 17 alpha estradiol and not the 17 beta estradiol.
Since its the 17 beta estradiol that is 100X more feminizing than the 17 alpha estradiol I was thinking this would be a good thing to monitor (easier and faster acting than having to check to see if your breasts are growing too large I don’t want to wake up one day with Double D boobs…
So this brings up the entirely new question of whether the estradiol blood test discriminates between 17 alpha estradiol and 17 beta estradiol. Perhaps someone here has some experience with these blood tests and can shine some light on the topic for us…
I was wondering about the difference : Are you thinking the accurate test is only sensitive to 17-B-E while the regular test can’t differentiate 17-A-E and 17-B-E ? Was the test results you posted for the person in the video ? That person in the video was only taking large amounts of 17-B-E cream, so that is not the result I would expect.
I would love to be able to test 17-A-E and 17-B-E separately, but Boldi’s experience with using 17-A-E suggests that the normal test responds to both types of Estradiol.
Ah - good point, I had forgotten about that post by @Boldi . It seems we should be checking for IGF-1 levels too. But given the estradiol test doesn’t seem to differentiate between alpha and beta, I guess its only value is telling us whether its getting absorbed…
Yes, I think the accurate test can measure 17-B-E accurately and not mix it with 17-A-E.
His Estradiol normal test measured at 36.8 pg/mL while the sensitive one was 9.9. Basically from a top percentile in 17-B-E levels to a low percentile, in terms of accuracy. The other video was just for general info.
Gyno can probably be reversed for most if it is treated within 1-2 years, pref earlier, with a SERM (selective estrogen receptor modulator) like Raloxifene, if it would happen. Of course for some it wouldn’t work and would require surgery. If 17-B-E did increase or the 17-A-E did cause it by some other mechanism. Also I don’t think it would grow that fast, you would notice it, lol.
OK, looks like I definitely want to do the at least the sensitive test, or possibly both versions.
It is still not clear that Labcorp’s version of GC/MS is actually able to distinguish 17alpha-Estradiol, but it is worth checking. This paper from 2010 lays out a GC+MS/MS method to test for both Isotopes, using sample handling similar to what Labcorp might do, but it is not clear if it is the same method used by Labcorp :Simultaneous measurement of 17-A-E2 and 17-B-E2 by GC + MS/MS
Googling on the net I just stumbled on yourholisticdoc.com, that offers Labcorp & Quest based testing at typically half the price of LEF : For example the Estradiol (high sensitivity) test is offered for $29.75 (vs $60 for LEF), IGF1 for $27 (vs $75 for LEF). Not all tests are cheaper : DHT is $114 (vs $50 for LEF). Seems to be small holistic practice, that somehow has access to Labcorp & Quest discounts not available to the much larger LEF.org. I just placed an order for Estradiol(HS) + IGF1 + LH+FSH + Testosterone for $138.25 : will see if they actually email me a Labcorp Requisition.
LC-MS is less likely to have false positive results for 17-alpha-estradiol than GC-MS, because it does not require derivatization of estrogens before analysis¹. LC-MS can separate and detect estradiol and 17-alpha-estradiol based on their mass-to-charge ratios and retention times².
However, LC-MS may still have some interference from synthetic estrogens or endocrine therapy drugs that have similar structures or masses to estradiol and 17-alpha-estradiol². For example, ethinylestradiol (a synthetic estrogen used in oral contraceptives) may mask lower level estrone (another estrogen hormone) peaks at very high concentrations².
Therefore, LC-MS can avoid false positive results for 17-alpha-estradiol if it uses a proper sample preparation and chromatographic separation technique. It can also use tandem mass spectrometry (LC-MS/MS) to increase the specificity and sensitivity of estradiol testing¹³.
The sensitive estradiol test using LC-MS/MS is less likely to falsely report higher estradiol levels due to an increase in 17-alpha-estradiol than immunoassay tests, because it can separate and detect estradiol and 17-alpha-estradiol based on their mass-to-charge ratios and retention times⁴. However, it may still have some interference from synthetic estrogens or endocrine therapy drugs that have similar structures or masses to estradiol and 17-alpha-estradiol⁵⁶.
For example, a study by van Uytfanghe et al. (2020) found that only at very high concentrations (2000 nmol/L) were 17-alpha-estradiol and ethinylestradiol peaks found to mask lower level estrone (E1) and estradiol (E2) peaks, respectively⁵. They also reported that their ultrasensitive LC-MS/MS method was suitable for routine assessment of serum E1 and E2 levels in breast cancer patients during estrogen suppression therapy⁵⁶.
Therefore, the sensitive estradiol test using LC-MS/MS can avoid false positive results for 17-alpha-estradiol if it uses a proper sample preparation and chromatographic separation technique. It can also use tandem mass spectrometry to increase the specificity and sensitivity of estradiol testing⁴⁵⁶.
We might want to have a bing chat / chatgpt thread for all content generated by LLM’s on all topics? I don’t want to spam this thread with bing chat info.
Sex differences- the fundementals for exasperating autoimmune are similar in both sexes, generally speaking. The difference is we don’t have the genetics to express dense receptor sites along with high levels of endogenous female specific hormones, other complexities. Though, GI specific autoimmune conditions have different fundamentals than systemic and in the case of Crohn’s, it could be helpful, but I can’t be sure. I am aware that Crohns and Colitis are different diseases but fundamentals are similar. Furthermore, there’s many studies on ER Alpha and GI diseased states.
Estrogen-related receptor alpha (ERRα) is a key regulator of intestinal homeostasis and protects against colitis
Astaxanthin was a success in the ITP, but it’s contradicted in “autoimmune diseases”, again because fundamentals are generally the same. If I take 12mg, I’m feeling it the following day.
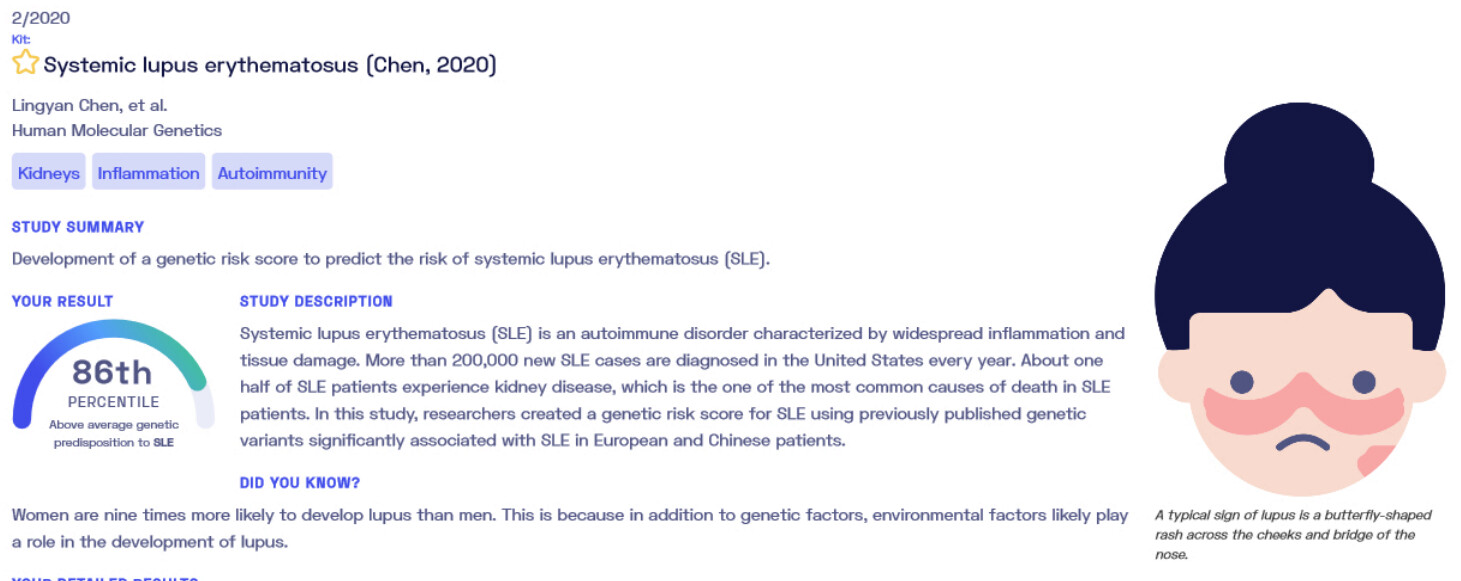
I have 86th percentile for lupus genetically for one study, however I don’t think I have lupus, or is it a spectrum where there are different degrees? Would I notice side effects from 17-A-E and then I could stop it? I had butterfly rash when I was a kid.
Yes, you are at increased risk beyond lupus based on ER Alpha. It’s not so cut and dry, many variables to account for, with many unspecific autoimmune attacks based on the risks with aging alone. Think beyond “lupus” based on the fundamentals and risks, it’s far beyond that. It’s difficult to measure tissue and organ attacks where it matters vs. what’s easily measurable- serum markers which predictively that would be my biggest concern. You cannot reply on serum or subjective symptoms, to measure risk of damage- that’s the biggest mistake for these patients.
I think it’s important to note that we have other agents that meet hard end-points for personal experimenting namely- rapamycin, SGLT2, acarbose, statins, ARB/ACE, otherwise synergy with controversial compounds NAD+, metformin (even for synergy with rapamycin), D+Q etc. lots of choices here.
On a large population scale and better said for the “average person” there are still hypothetical risks with some of these combinations above. I’m not 100% confident in the combination of SGLT2 and rapamycin in humans.