If true, this is only the case in the US. In systems with socialized healthcare (covering the vast majority of the world’s population), this is not a factor at all. I think herd mentality is more influential. And herd mentality creates effects of scale: most doctors prescribe losartan over telmisartan, so more losartan is produced, so losartan can be made for cheaper (effect of scale) and can be available more broadly at all local pharmacies (network effect), so more doctors prescribe losartan => rinse and repeat. (And add to that the “brand” effect.)
The average American in the private sector holds a job for 3.7 years That means that on average, insurance companies are going to churn you every 3.7 years or sooner if your company changes the insurance plan. Their incentive is to cover you only in two categories of things. (1) Things that pay themselves back in less than 3.7 years. (2) Things that have such an overwhelming demand from employees that their employers think that they absolutely have to cover them to stay competitive.
If the only advantage of telmisartan is a reduced rate of dementia in old age (so waaaaay more than 3.7 years later) and if telmisartan is a bit more expensive than losartan and if patients are not aware of telmisartan’s benefits over losartan then there is ZERO financial incentives for any insurance company to promote telmisartan over losartan.
It is reasonably priced at $10 per month. It will do most of the work for you in finding papers and summarizing the results. You can also ask it many different medical questions and unlike Chat GPT it always provides accurate references.
FYI, I just sent this to my doctor, who is brilliant and up on most longevity medicine, and he said he’s been using this for a while and it’s really good!
What I was really was talking about is an AI built in to my EMR. So it can also generate differentials, ICD codes, diagnosis, SOAP notes, consultation letters, etc…
First, it is true. Second, I don’t know about every country, but I’ve worked in government health systems and the process is similar but the government decides for everyone which medicine will be provided, usually based on cost.
I don’t know where you worked but in countries I know (France, the UK and Turkey) doctors can prescribe any approved drugs (for the approved condition), no matter their price. So even though telmisartan is more expensive than losartan, doctors can prescribe it and patients will then get them from the pharmacy for free or very little: in Turkey it’s almost free, in the UK it’s a fixed price (independent from the drug price) and in France the gov pays 65% of the drug price and then private insurers (all employees have one) pay the rest. So when Dr. Bart wrote “THE MOST INFLUENTIAL FORCE ON DOCTOR DECISION IS…DRUM ROLL… WHAT IS COVERED BY THE THIRD PAYER…”: no, it doesn’t apply to these countries. And from what I read most other countries in the world follow a model similar to Turkey (free), the UK (low fixed price) or France (%).
This is a very important distinction. Hospitals are extremely price sensitive and they have very short-term incentives (a few days until you leave). So they will almost always prefer the cheapest drug. In France I was told that some hospitals start buying drugs in bulk abroad (I assume from other EU pharmacies) or to give off label drugs to save on costs.
It’s very common for hypertension only to be discovered during a hospital stay. The hospital gives a drug and unless the patient complains of some side effect the GP will keep it. It happened to my grand mother a few months ago: hospitalized for a pneumonia, high BP discovered, they gave her amlodipine 10 mg, she was discharged, she developed big edema, complained to her GP who said “it’s a normal side effect of the drug it means it’s working”, I pushed her to see a cardiologist to change amlodipine for telmisartan (or reduce the dose and add telmisartan), the cardiologist agreed that amlodipine 10 mg monotherapy wasn’t a good option for an 85yo woman but he replaced it with an ACEi unfortunately…
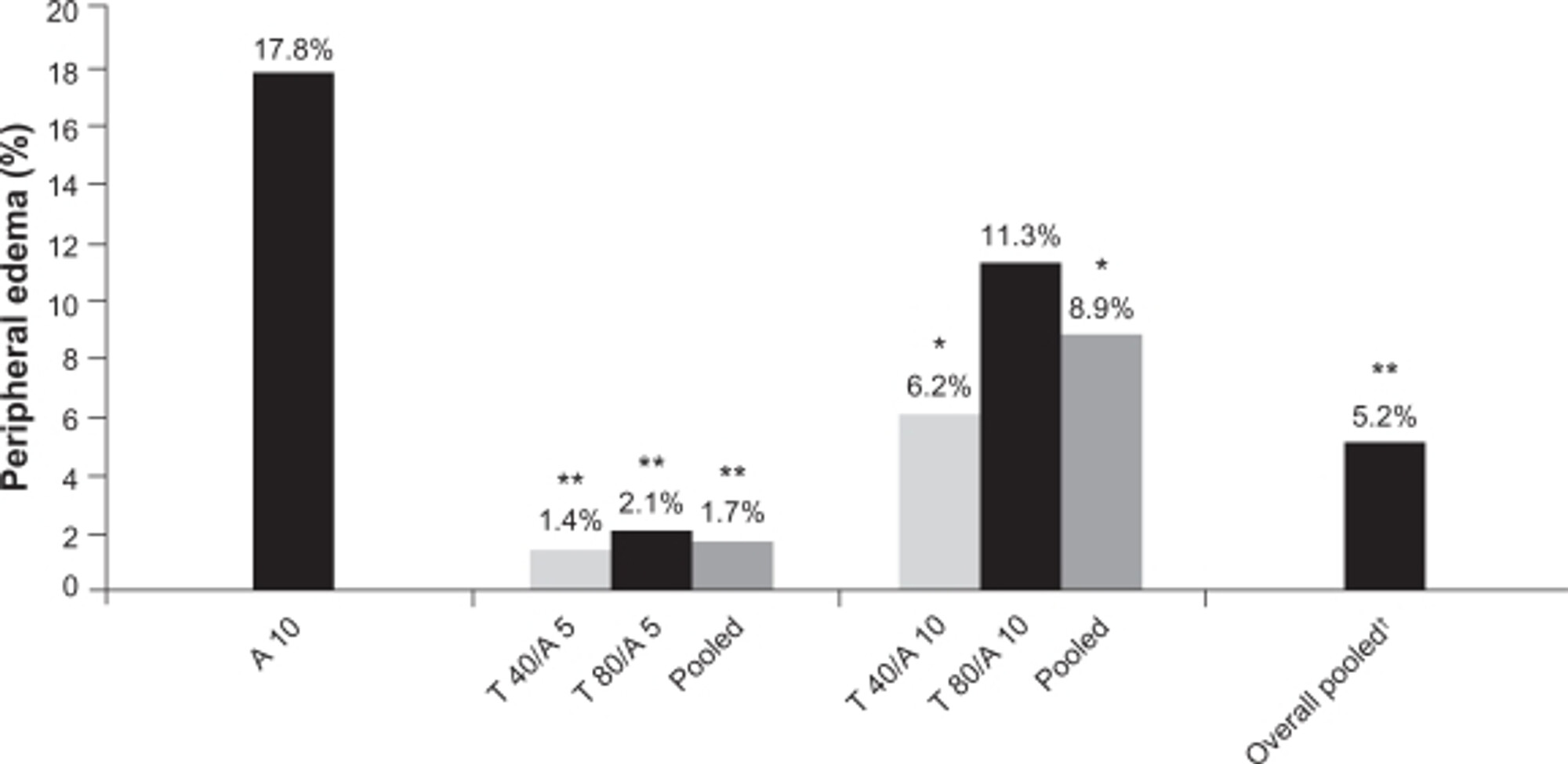
Amlodipine is a great drug (here’s why: Amlodipine in the current management of hypertension 2023). But taken alone at the highest dose, it has high rates of edema, especially in older women. In case of edema, one solution is to lower the amlodipine dose to 2.5 mg or 5 mg and add telmisartan (or probably any ARB), and you get edema rates close to placebo (if not lower):
Personally with my own health I’m doing Telmisartan 80 mg as I think we need at least that dose for PPAR and 5 mg of Amlodipine. I’m goaling average systolic of 115 mmHg.
My current assessment of the literature is Telmisartan first, take it up to 80 mg, then if something needs to be added Amlodipine up to max of 5 mg, then if something needs to be added then indapamide.
Important note if needing to add indapamide it takes 4 weeks to get 60% of the benefit and 8 weeks to get full effect. But also some people will drop their sodium or potassium level of affect their kidney function, so all of this requires ongoing monitoring by one’s physician.
I want to mention that TELMESARTAN CROSSES THE BLOOD BRAIN BARRIER and of the ARBs it and Candysartan are the only ones that do. I have used Telmesartam 80 mg per day for 9 years. I use amlodapin occasionally if needed or 40 mg of coal is as my pulmonary artery is borderline elevated. Am on Rapamycin 6 mg once a week for 6 plus years am 89 and in training for the pole vault in the master track program, Rapamycin has caused my dangerously expanding aorticring to shrink fr 5.1 cm to 4.1(now normal). There are 2 studies in Asia showing this can happen in rat models of this disease… GBEST MD retired anesthesiologist.
I know this is a post from May but only saw it now. An aortic root reduction from 5.1 to 4.1 is incredible and saves you from open heart surgery. Assuming this was measured via echocardiogram, the measurements can change depending on who is measuring but a whole 1cm reduction is impressive considering an aortic root only grows more once it reaches a certain size.