Hey it seems to work in Turkey.
Interesting that Turkey is so under-doctered. They have a third the number of doctors as Greece. Their life expectancy is about 4 years less. I wonder if any studies have been carried out on thus.
2 Likes
The rhetorical question “doctors or pharma” asked by the podcast host was to show the enormous value brought by big pharma despite their tiny share of healthcare spending (13%). To this rhetorical question, I’d answer “pharma” without hesitating. I don’t even see how this can be debatable. With the best doctors in the world, but without drugs, we would have a way lower life expectancy. (And anecdotally, many people here seem to do well with good drugs while bypassing doctors.)
Then, are doctors even good at generating a differential diagnosis? Medical errors are the third cause of death in the US and AI already makes better diagnoses than doctors.
Indeed, when we look at various countries, above about one doctor per 1k inhabitants, there’s no association with life expectancy:
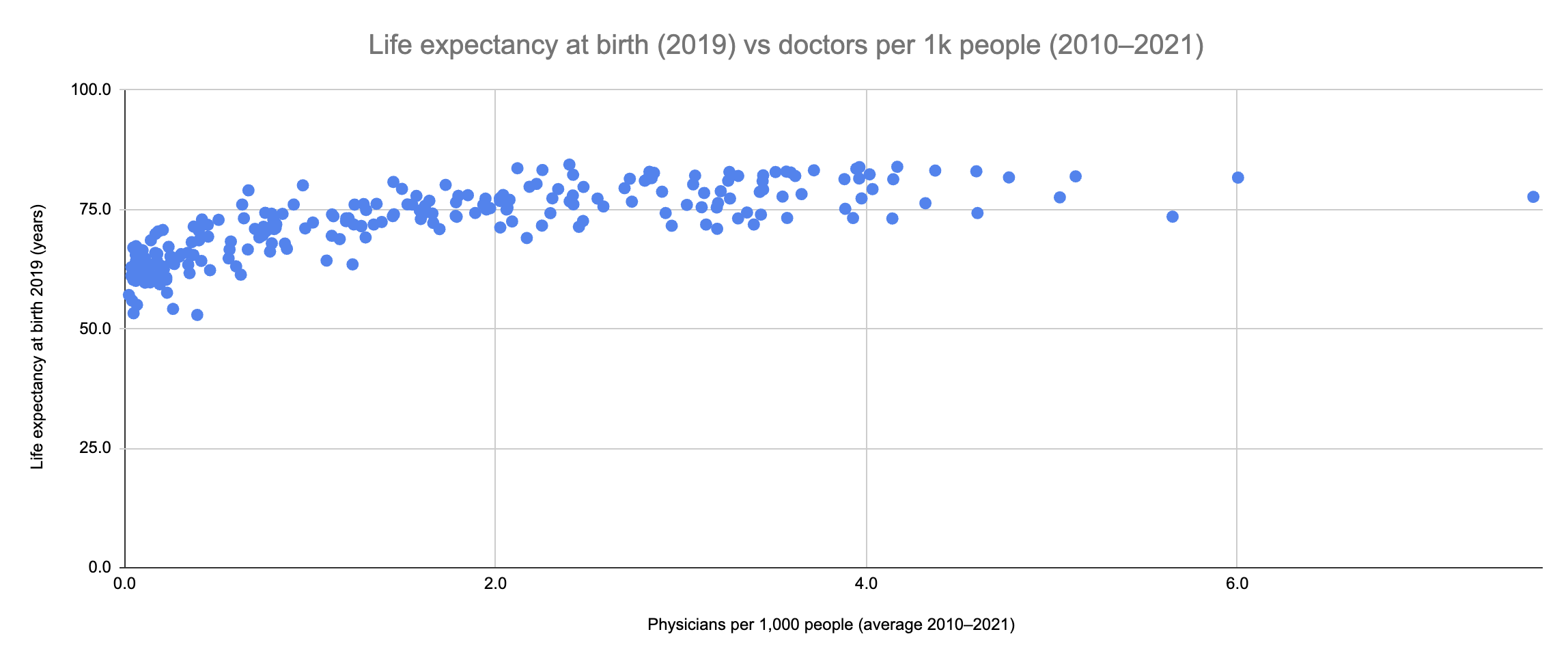
Data from the World Bank, I took the 2019 life expectancy before the Covid dip (but I assume the results would be identical): GDP vs Life expectancy vs Doctors - Google Sheets
Turkey is a good example indeed: 2 physicians per 1k people vs 3.6 in the US and 4.3 in the EU. Nominal GDP per capita $11k vs $37k in the EU and $76 in the US. And yet life expectancy: Turkey 76y, EU 80y and US 76y. But Turkey has access to the same pharmaceutical miracles brought to us by big pharma.
My (soon-to-be) in-laws are Turkish doctors and hospital owners, and my fiancée has a medical tourism business bringing European and American patients to Turkey. I’ve been treated in Turkey myself, and I can confirm that the healthcare system there is 10x better than in France (where I was born and lived most of my life) and the UK (where I’ve been living for the past 3y). I attended meetings in London with my father-in-law (a radiologist, who wanted to open a branch in the UK) and British NHQ doctors, and the Brits were shocked by:
- The quality of the equipment in Turkey (latest device, world-class in Turkey vs some old machines in the UK, at least in NHS clinics),
- What is offered to people, for instance at most 2 ultrasounds for pregnant women in the UK (NHS) vs every month in Turkey (in the public healthcare system),
- The supply: you get an appointment in a few days in Turkey (if not on the same day) vs after months with the NHS.
(btw, if you want cosmetic or longevity treatments or checkups in Turkey, lmk)
I was also impressed by the Turkish healthcare IT:
- Every single medical act (whether it’s done in the public or private sector) is registered in a central database and all Turkish people have access to a national healthcare portal (e-Nabız) where they can see prescriptions, test results (I think you can plot them over time), MRI images, etc.
- When a doctor prescribes you something, it’s a digital prescription attached to your ID card, so you can go to any pharmacy in Turkey, show your ID card and the pharmacist gets the prescription from the system and gives you the prescribed drugs (for “free,” ofc).
Westerners don’t realize how bad their healthcare system is until they go to “developing” countries. These countries have less money and fewer doctors but achieve better results (as measured by life expectancy) because they leverage tech and drugs.
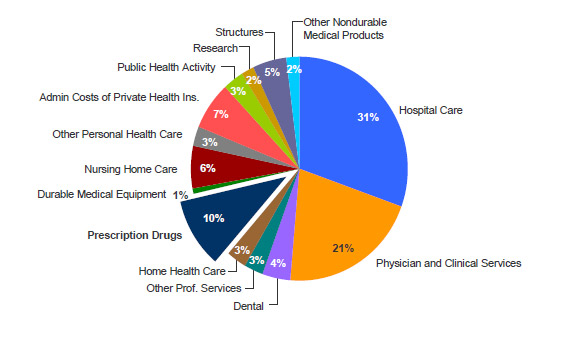
Anyway, here’s the breakdown of healthcare spending in the US (source):
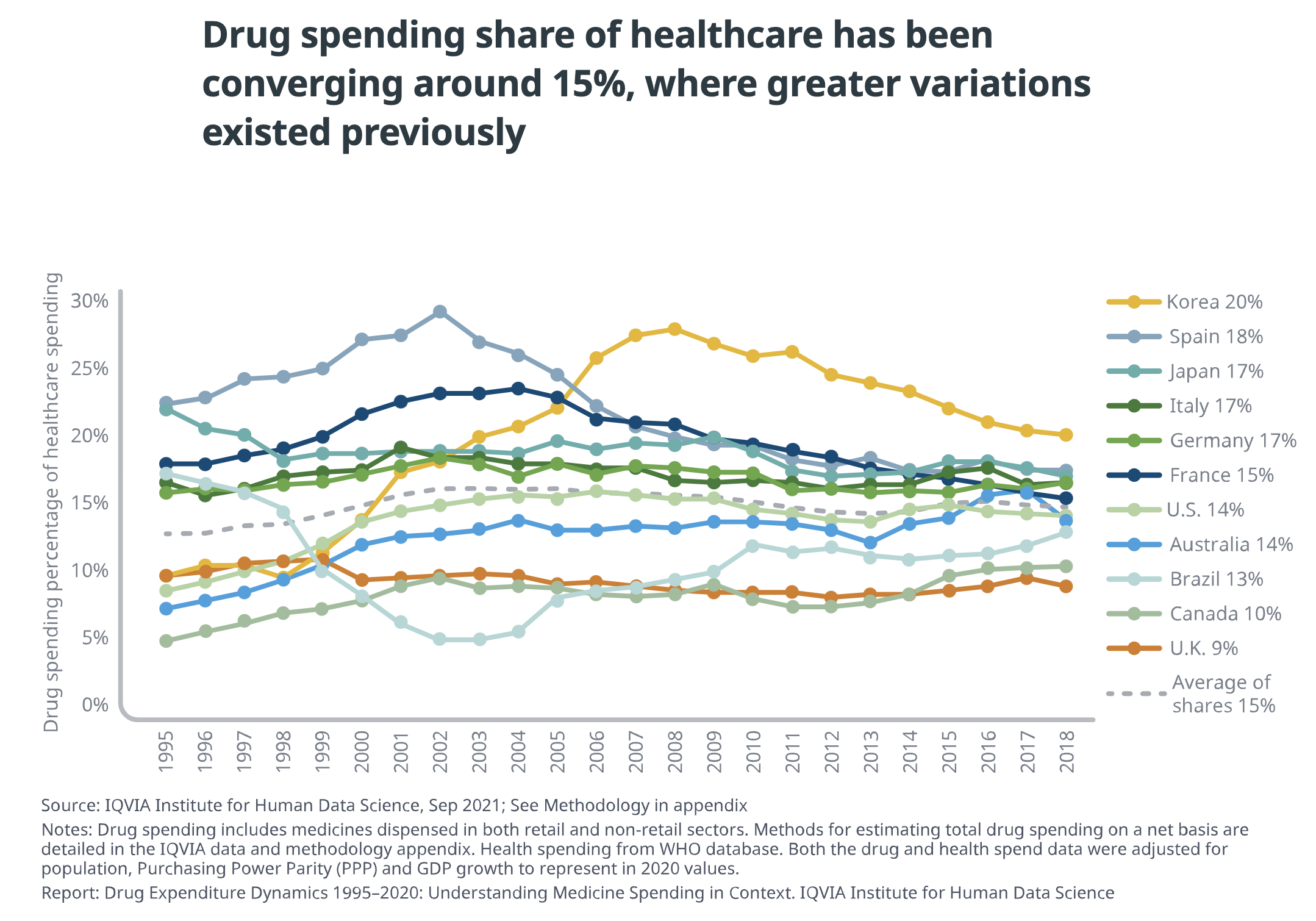
It seems to be around 15% around the world and fairly constant (source):
What about profits? Here are the Return on Capital (ROIC):
- Healthcare Support Services: 45.74%
- Hospitals/Healthcare Facilities: 20.16%
- Healthcare Information and Technology: 14.28%
- Drugs (Pharmaceutical): 13.38%
- Healthcare Products (I guess it means medical devices and other non-drug medical products?): 13.08%
- Drugs (Biotechnology): 1.56%
- (US average across industries, without financials: 14.70%)
So big pharma’s profits are lower than average and they represent a small part of total healthcare expenditure, while medical staff (doctors, pharmacists, nurses, etc.) represent the majority of the spending and are swimming in cash with higher than average profits.
But big pharma is bad because they lobby? Think again. In the US, according to Open Secrets, total spent in annual lobbying:
- Pharmaceuticals/Health Products (Pfizer, Amgen, etc.): $378,585,382
- Hospitals/Nursing Homes (American Hospital Association, HCA Healthcare, etc.): $131,012,728
- Health Services & Health maintenance organizations (UnitedHealth Group, Kaiser Permanente, etc.): $126,810,968
- Health Professionals (American Medical Association, American Academy of Family Physicians, etc.): $93,471,087
So “Pharmaceuticals/Health Products” represent 51% ($378,585,382/$739,055,454) of all health lobbying spending in the US. Same as nurses and doctors (as the main cost of “health services” is the medical staff). And actually, if you look at “Pharmaceuticals/Health Products” they put in this category the “Pharmaceutical Care Management Association” representing the corrupt PBMs (so not big pharma) and generic manufacturers like Teva. They also included device manufacturers like Abbott Laboratories and Medtronic Inc.
Conclusion: doctors represent a larger share of healthcare spending than pharma, they make more money than pharma, they spend more on lobbying than pharma, they’re not associated with an increased lifespan, and they can be replaced by AI.
Quod erat demonstrandum.
10 Likes
that’s a brilliant graph, thank you.
You make interesting points. And i suspect you’re right that if we had to lose one we should lose doctors not drugs. If the question is: would we be better off getting rid of doctors and spending the money on a bigger drugs budget/r&d, then the answer may be different. There may be dramatic diminishing returns from spending more on drugs or r&d than we currently are
I did think of some issues with your argument, but i don’t pretend to be able to prove the counterargument.
The issues i can think of
- The association may be confounded by diet and lifestyle. Eg. Wealthier countries tend to have more doctors and more ultra processes food.
- Much of healthcare, esp nurses etc isn’t necessarily reducing morbidity, it is also improving the conditions and lives if very sick people. In many countries any slack In care is taken up by families.
- AI replacement, I’m pro aggressive use of AI, but much of the trialling uses younger volunteer patients and so may misrepresent real world use in elderly etc.
I suspect the answer is that expensive western healthcare has been skewed towards critical care and secondary care. Which is less value for money than primary and preventative care. Preventative drugs no doubt provide the best bang for buck. But telling the family of a cancer patient that it’s not economic to provide care is unviable in a western democracy now we’ve had our expectations raised.
2 Likes
Regarding the issues you mentioned:
- Confounders like diet and lifestyle: maybe. However, if we still consider Turkey, they have more diabetes than the US and a similar rate of obesity. So their diet and lifestyle aren’t amazingly great. And despite that (and being 7x poorer than Americans with 2x fewer doctors) they have the same life expectancy as in the US!
- True that part of healthcare is to have a better “patient experience” that may not have any impact on your health and life expectancy. That being said, from my experience in Turkey, the level of care and user experience there is 10x better than in the UK and France. My grandparents were hospitalized a few times in France, when my Turkish fiancée visited them with me she was shocked by how hospitals were, the lack of staff, etc. And these were good public French hospitals in wealthy neighborhoods in Paris. Really, that made me wonder where the “Third World” was…
- Yes, AI isn’t ready yet for use. But it’s already massively used… by doctors themselves! (according to friends who are interns in emergency rooms at least, so anecdotal example)
And yes definitely for critical sick care vs preventive healthcare. Actually, here, the incentives of big pharma are probably more aligned with ours (as customers) than those of doctors and hospitals. Example: If you start intensive lipid-lowering therapy at age 30. Low cost for you (generic statins), but you’ll probably never see a cardiologist in your life (or at least not every 6 months for a checkup as my grandpa does) and never be hospitalized for a major adverse cardiovascular event. So in terms of $, you’re a net positive for pharma (small but regular income over your lifetime, and actually they want you to live longer to keep buying statins) while net negative for doctors and hospitals.
5 Likes
See today’s news report in STAT:
The trove of documents, which was released as part of a legal settlement with the state of North Carolina, shows that Juul tried everything from orchestrating untraceable political donations to paying think tanks for favorable research, in an effort to revamp its image and prevent both Congress and the FDA from taking action that could cost the company financially.
The strategies aren’t necessarily surprising themselves, transparency advocates told STAT. But it is rare to see them laid out like this.
“It isn’t often I get to look at this whole pool of influence peddling … being used by one company, even though I know it happens frequently,” said Craig Holman, the government affairs lobbyist at Public Citizen. “It surprises me to see it, but I know it happens.”
…
Juul’s internal documents provide rare insight into how corporations use so-called dark money groups to funnel large donations to political candidates.
According to an internal spreadsheet entitled “Political Giving Strategy,” Juul considered writing six figure checks from the company’s treasury to several so-called “social welfare organizations” as a means of influencing congressional leaders. Unlike other political donations, corporations aren’t required to disclose their donations to these sorts of organizations, known as 501(c)(4)s.
…
Internal budgets reveal that by April 2019, Juul was forking over more than $200,000 per month to “strategic advisors” — former staffers for Presidents Obama and Bush and powerful members of Congress like Schumer who played an integral role in charting Juul’s strategy in Washington.
today in STAT:
3 Likes
When buying and selling are controlled by legislation, the first things to be bought and sold are legislators. — P. J. O’Rourke
5 Likes
what is the average wait time for specialists in Hong Kong?
I am definitely interested in learning about longevity checkups and treatments available in Turkey. Is there a website you could recommend for initial research or is it better to DM you?
The average wait time for a specialist is usually a few days. There are some that are booked up for months though. For instance my annual checkup needs to be booked at least a month in advance.
1 Like
It reminds me of this Onion humor (you have to laugh, or you’d be crying):
Citing a desire to gain influence in Washington, the American people confirmed Friday that they have hired high-powered D.C. lobbyist Jack Weldon of the firm Patton Boggs to help advance their agenda in Congress.
“Unlike R.J. Reynolds, Pfizer, or Bank of America, the U.S. populace lacks the access to public officials required to further its legislative goals,” a statement from the nation read in part. “Jack Weldon gives us that access.”
“His daily presence in the Capitol will ensure the American people finally get a seat at the table,” the statement continued. “And it will allow him to advance our message that everyone, including Americans, deserves to be represented in Washington.”

4 Likes
If they are as good as the dentists that work in turkish dental tourism I’d avoid them like the plague…
1 Like
I go to Turkey for dental treatment and it’s better (and cheaper) than in France and the UK. I know that the British Dental Association pays a lobbying and PR firm to identify the few patients that had problems in Turkey and then publish news articles about them. Is there a higher rate of medical malpractices in Turkey vs the UK? I’d say no, but do we have data on that? Otherwise it’s just hearsay.
Anway @essexaid here’s my fiancée’s website: https://www.treat-away.com They mostly do cosmetics (and they have NHS nurses among their patients, which is quite telling…) but feel free to contact them to enquire about anything else. Some longevity clinics are opening there. (Of course as it’s my fiancée’s business I’m biased, so usual caveats: not medical advice, do your own research, etc.)
2 Likes
No it’s not it’s atrocious but of course they do it in a way that patients can’t tell the damage done to their teeth. All my many patients that went to Turkey for dental work were treated by scumbags that intentionally tried to hide to bad work they did. Here an example of a very satisfied customer of Turkish dental work. I have many more such examples but the crowns are B1 or glow in the dark white even and all look "perfect " so the customer is satisfied…
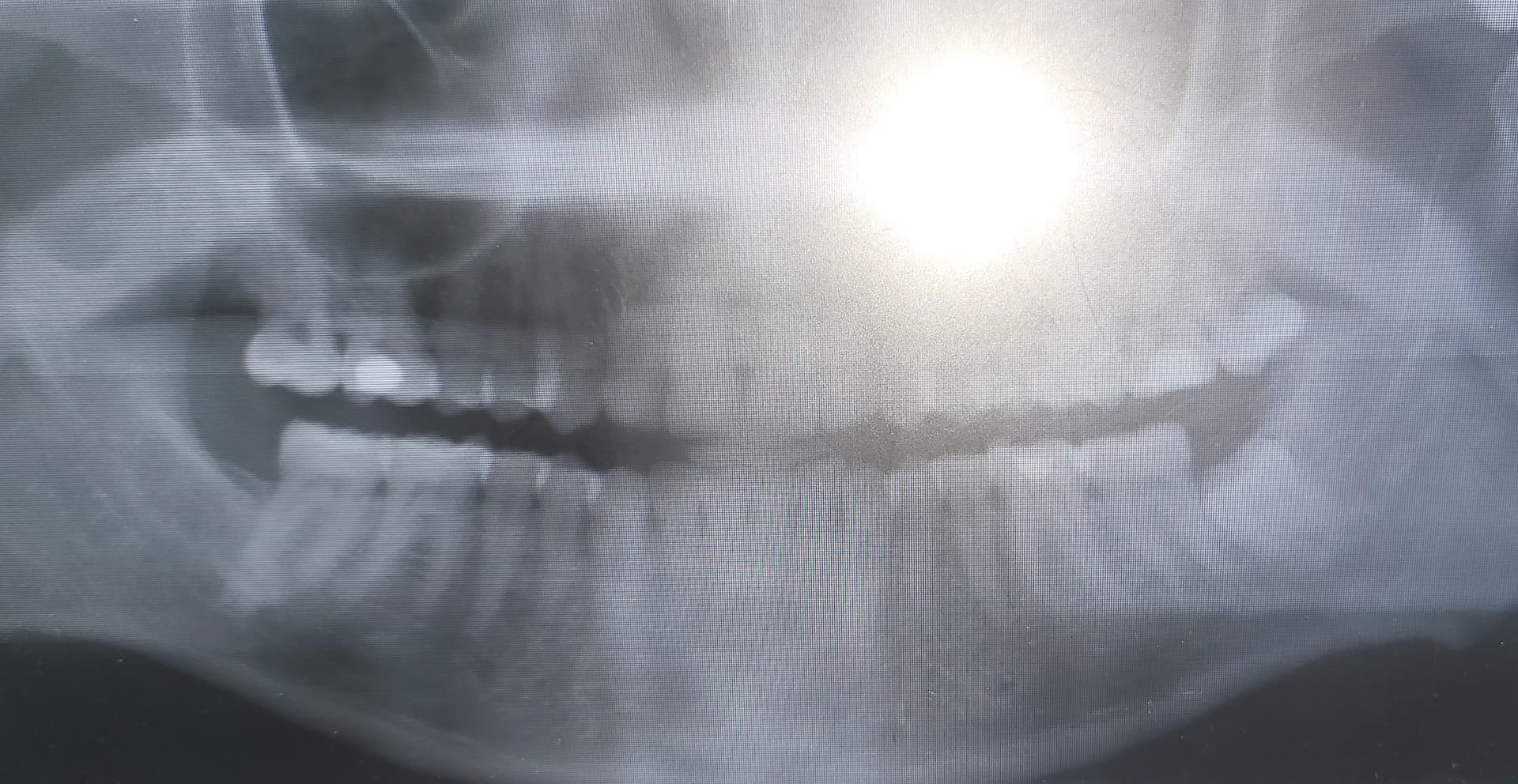
I’ve seen quality work from Thailand and the Philippines but never from Turkey, Eastern Europe, the Levant nor Maghreb but I have seen many many problems caused by poor dental work from there…
Thank you @adssx and @Arhu for your views, I value them both and shall certainly investigate further.
Surely all dental treatments done in Turkey are “atrocious” and all Turkish dentists are “scumbags”. Maybe all Turks, actually?
Fwiw, all Turks, Lebanese, and Eastern Europeans I know in London (including HNWIs and UHNWIs) go back to their home country for medical treatments, and especially for dental treatments. I assume they’re satisfied with the work done there, even after decades. On the other hand, you might suffer from selection bias as I would assume that unsatisfied patients tend to come and see you more than satisfied ones. Still, there are butchers in Turkey. As everywhere else. And foreign patients are more likely to be scammed than locals. As everywhere else. Unfortunately, it has more severe and irremediable implications when it comes to dental surgery versus buying a fake bag in the bazaar. That’s why people willing to embark on a medical tourism journey should do their own research and know the risks. Despite these challenges, medical tourism is quickly growing around the world:
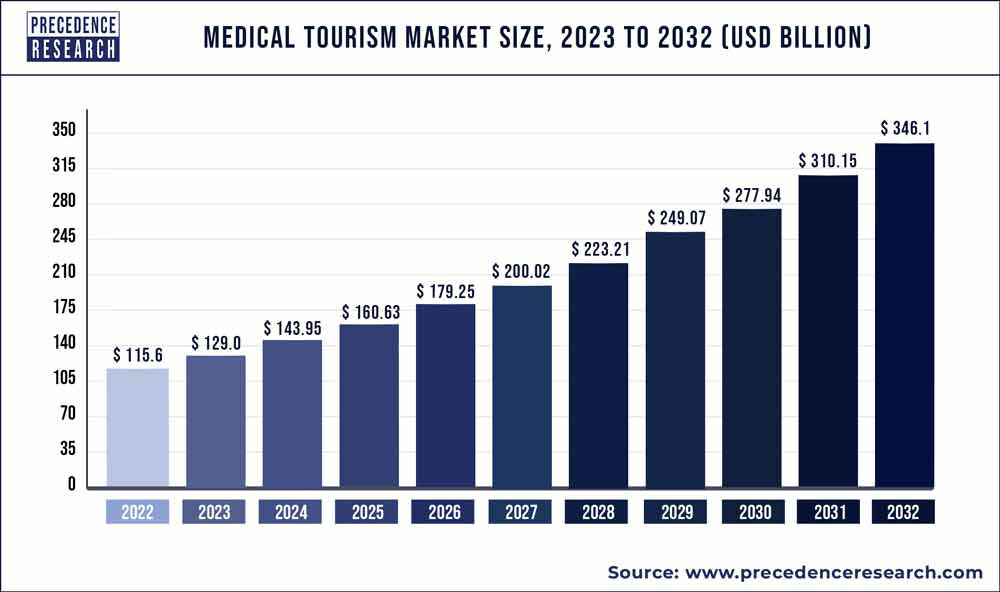
4 Likes
They go home because they think they are getting a better deal and like you cannot judge the quality of the work done. The big problems only arise 5-10 years later
2 Likes
Haha. Cope harder. As I wrote, “even after decades”. Damned, I’m talking about actual multi-millionaires, but somehow, you seem to know every single doctor in Turkey, Lebanon, and Eastern Europe to be able to give a conclusion.
2 Likes
Let’s avoid general sweeping comments.
2 Likes
Yes - and no ad hominem attacks.
Its fine to point out issues in someone’s arguments, but lets not get personal on things. Go hard on the science, easy on the people.
2 Likes