I didn’t know. Why is BA not easily available?
In EU it is Daiichi Sankyo Europe that is going to market it, I don’t know where you can get it.
The partnership continues to grow, with DSE recently gaining approvals for bempedoic acid in the Netherlands, Slovakia, and Spain.
https://www.businesswire.com/news/home/20240103960094/en/
1 Like
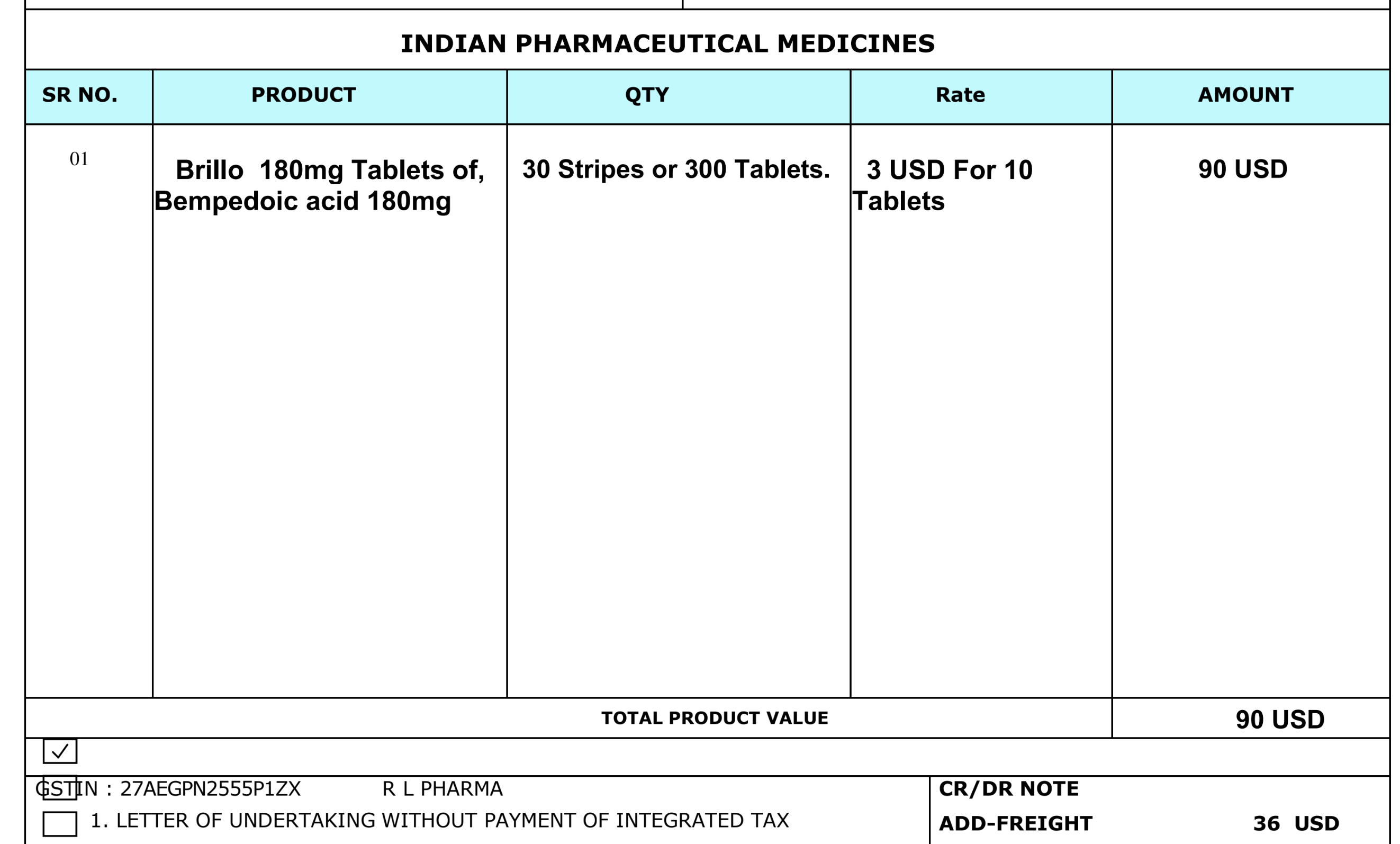
Bempedoic is available from any Indian supplier that you are comfortable with.
I ordered from India.
My current lipids are quite good but could use some tweaking.
My stack will be atorvastatin+bempedoic acid+pantethine.
After using it for a couple of months I will get tested and see if bempedoic acid makes any improvement. Currently, I am on atorvastatin+pantethine, which causes all of my lipids to be in the “desirable” range according to Quest Labs.
1 Like
I’d guess the bigger issue is mitochondria issues caused by the statins. Brains are big users of energy.
quote=“Bicep, post:4, topic:11746”]
Thus, endogenous low molecular weight compounds such as cysteine, arginine, glutamate, citrate and glutathione, as well as proteins are metal-binding agents.
[/quote]
Zeolite is supposed to work too.
I quoted a paper here that I posted in “chelation for heart disease”. Apparently heavy metals, especially lead is bad for heart disease. These metals are not usually in circulation so I don’t see how they can be removed without chelation. I don’t know what the mechanism is but EDTA or DMSA chase the metals out of surrounding tissue and tie them up.
If you don’t have heart disease it probably isn’t worth it to do just to find out, but I don’t know any other way.
1 Like
Peter Attia believes (paywall) statins negative effect on diabetes risk is due to inhibiting HMG-CoA reductase in muscles, which are a sink for glucose and plays a large part where statins are displaced. Anyone who has muscle side effects he doesn’t see a problem with CoQ10 supplementation, which might help, possibly from placebo effect.
In a small study CoQ10 supplementation showed a significant improvement in HOMA-IR, basically insulin resistance:
One of my hands is slightly messed up, but I’ve had this problem for years and with other supplements, so I might try CoQ10 if statins have an effect.
But since statin usage is both associated with and causally linked with a decrease in all-cause mortality, the benefits outweighs the risks:
The risk of all-cause mortality was significantly reduced in statin users (hazard ratio: 0.72, 95% confidence interval: 0.66–0.76).
See the super tight CI as well.
1 Like
I don’t think this review has been posted here (but I may have missed it):
Effect of statins, PCSK9 inhibitors & ezetimibe (cholesterol-lowering therapies) on all cause mortality.
From a 2023 metaanalysis of 60 RCTs in ~300,000 patients.
Extent of Low-density Lipoprotein Cholesterol Reduction and All-cause and Cardiovascular Mortality Benefit : A Systematic Review and Meta-analysis
Compared with placebo, usual care or less-intensive therapy, active or more potent lipid-lowering therapy reduced the risk of all-cause death [ARD −1.33 (−1.89 to −0.76); NNT 754 (529–1309); RR 0.92 (0.89–0.96)]. Intensive LDL-C percent lowering was not associated with further reductions in all-cause mortality [ARD −0.27 (−1.24 to 0.71); RR 1.00 (0.94–1.06)]. Intensive LDL-C percent lowering did not further reduce CV mortality [ARD −0.28 (−0.83 to 0.38); RR 1.02 (0.94–1.09)]. Our findings indicate that risk reduction varies across subgroups and that overall NNTs are high. Identifying patient subgroups who benefit the most from LDL-C levels reduction is clinically relevant and necessary.
7 Likes
Given that we already see plaque reversal at LDL-C levels far above 20-40mg/dL I am not surprised that further reductions do not show much additional benefit, at least not in the short term.
The benefit is exactly the same from decreasing LDL from 60 to 30 as if 100 to 70. Of course from 100 to 30 would have twice the benefit. On longer time scales it would be even higher.
1 Like
Interesting study that finds against the “lower the better” hypothesis.
This graph seems to encapsulate the key point that lowering ldl-c by more doesn’t translate to mortality benefit.
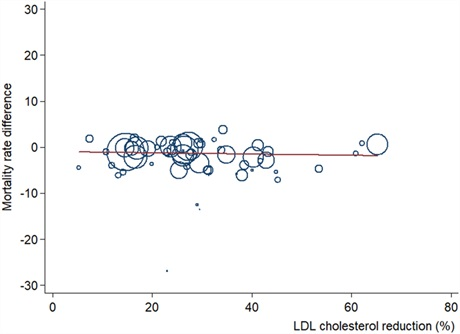
“WHAT THIS STUDY ADDS
Trials reducing LDL-C more than 50% did not consistently further decrease all-cause and CV mortality; the reduction in MI risk was consistent across all analyses.
Mortality benefits were found within trials with baseline LDL-C levels more than 130 mg/dL.
Achieved LDL-C levels were not related to mortality reductions.”
Interesting that they couldn’t find any benefit if starting ldl-c is already below 130mg/dl.
The idea that lowering apob or ldl-c confers the same benefit no matter where the start point isn’t supported by any intervention studies.
4 Likes
Yes, a 50% LDL reduction seems to have the maximum effect on all cause mortality. That’s taking an LDL of 120 down to 60, which is pretty darn good. I guess it just means that extra mile from 60 to 30 doesn’t really have the bang for the buck.
3 Likes
Yes, the meta analysis additionally finds this for cv deaths as well as ACM.
“Intensive LDL-C percent lowering did not further reduce CV mortality”
Driving LDL-C to ~60mg/dL and lowering inflammation with intensive statin therapy or dual statin/ezetimibe therapy may drive cardiovascular risk to near 0 even over many decades. Maybe a lifetime clinical trial involving millions of people would find a small, statistically significant acm in the statin+ezetimibe+PCSK9i group compared to the statin+ezetimibe+saline injection group.
If there was a cheap, oral PCSK9i I would add it to my stack but as of now I see no point in paying hundreds of dollars/euros for a monthly injection.
1 Like
Do we have data on LDL and mortality (all-cause or CV) but for a given total cholesterol?
For instance instead of a 2D plot a 3D one with LDL (or ApoB) as x and Total cholesterol (or HDL) as y and in z mortality.
3 Likes
Do you have a link to a study showing that there is a attenuation in the decrease in ACM at higher LDL reduction?
Most therapies can’t lower LDL above 50% so of course there isn’t enough data for that. Which reduces the statistical power.
I see that the case that most things said here and I imagine everywhere else is simply false, still holds true.
Absolutely pathetic for people to weaponize a lack of statistical significance like this. It’s dangerous. It’s evil. It’s misinformation. And I guess I have to call it out when I see it.
I have no problem trying to reduce LDL as low as possible. At some point the law of diminishing returns sets in. For me, that means I probably won’t pay the extra additive expense of a PCSK9i as getting to 60 should be sufficient for me. Spending a lot of extra money every month (as well as the inconvenience of an injection) to get a marginal improvement is not worth it for me personally. If others feel differently, that’s OK too. I’d rather skip the PCSK9i and spend $300 a month on other anti-aging treatments - Rapamycin, Empagliflozin, Lithium, etc…
I am using Bempedoic Acid, Ezetimibe and O3 fish oil as well as a healthy(ish) diet to lower my LDL as much as possible. If I could, I’d use a statin as well.
I think you would also agree that you get most of the benefits dropping from a high number (100-150) to a number half that size (50-75) for LDL. Is there a benefit to going lower? Maybe. Is it worth it? Not for me.
4 Likes
It sounds to me that you gave up and you are happy with having a suboptimal apoB. If that is your decision. I wouldn’t stop at PCSK9i but also look at other ways of lowering apoB further if you care about not getting atherosclerosis or heart disease for sure.
Some are clutching their 10-year risk calculators in one hand, and their magic crystals in the other, and are hoping for the best. I don’t know the difference.
This is interesting, an effect I was not aware of:
Effect of lipid-lowering therapies on C-reactive protein levels: a comprehensive meta-analysis of randomized controlled trials !
“Statins, bempedoic acid, ezetimibe, and omega3FAs significantly reduce serum CRP concentration, independently of LDL-C reductions.”
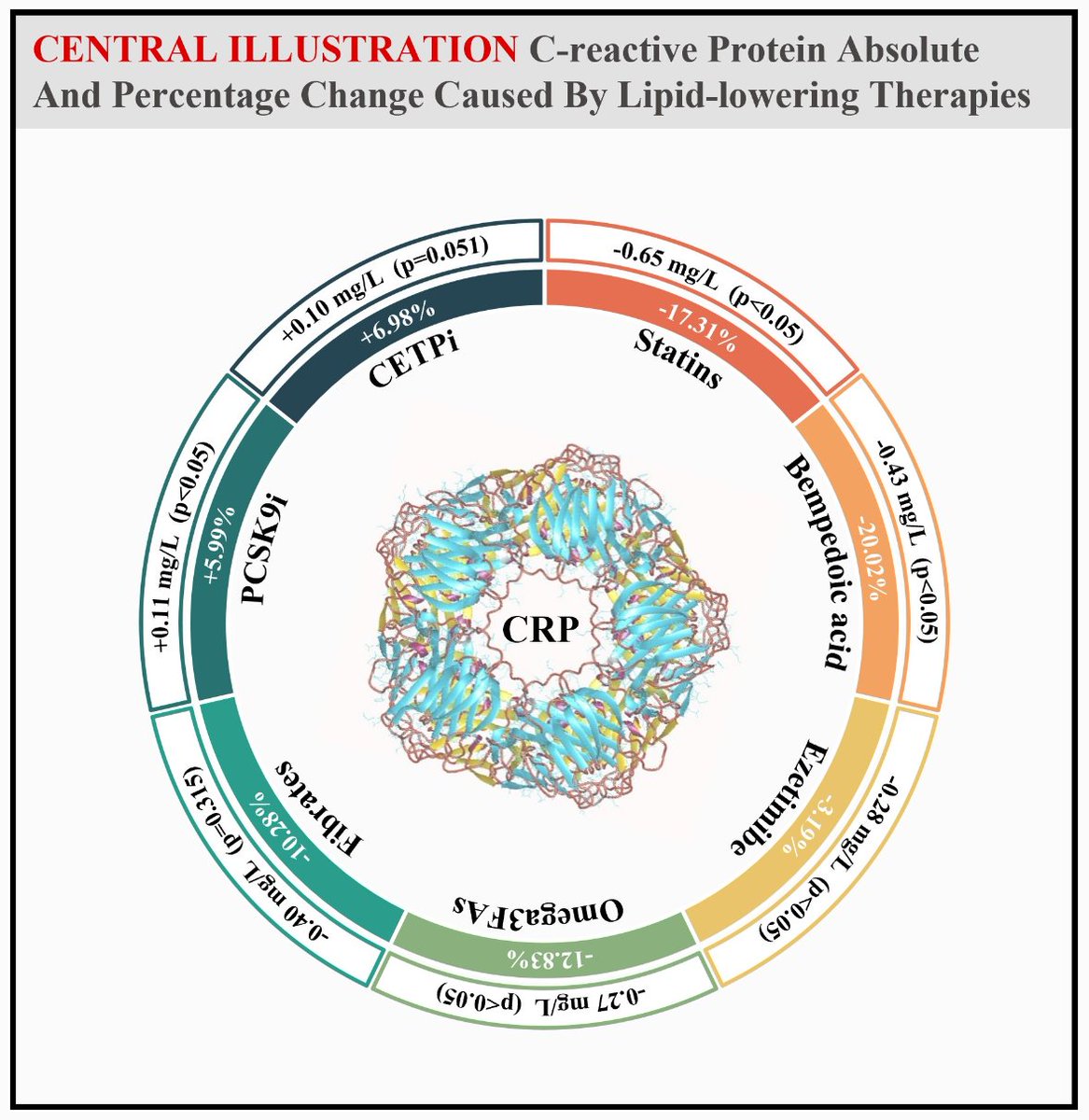
11 Likes
Yes, i don’t think there are any intervention studies in primary prevention that suggest you should go lower. The population association studies suggest you shouldn’t go lower, and the Mendelian randomization studie show a small absolute benefit “being” lower from natural genetics. Each type of study has limitations, but it seems that the various limitations of MR studies are the hardest for people to understand.
The idea that we can simply choose to have a lower apob is an obvious fallacy. We would choose an intervention, and that intervention would need to be used long term to bring benefit, and would come with potential side effects. These side effects of targeting vlow levels of apob haven’t been tested over the long term. So the side effects of using say, psk9i to go lower may easily outweigh any small absolute cvd benefits. We just don’t know from the evidence base.
It’s understandable that people fixate on cholesterol when they fear cvd, because it gives them a sense of control, but in reality death is a multi-factoral disease and longevity requires a multi-factoral approach. Even having your apob down at 30 doesn’t eliminate cvd risk. And if it comes at the expense of minor sarcopenia or minor mitochondrial impairment then the tradeoff may not be worth it.
4 Likes
This is an area I’m very interested in. The idea that statin benefits come from 2 mechanisms is intriguing. And I’m fascinated by the size of the bempedoic acid impact.
Does anyone know of any studies which show the dose response curve for statins on crp?
3 Likes