Yeah but a statin isn’t enough to me, and I don’t think statin + ezetimibe will be enough either.
Pitavastatin seems safe for hERG though:
Pitavastatin did not affect the hERG current but the lactone metabolite had weak effects on both hERG and action potentials of guinea pig papillary muscle at 3 µM. The lactone suppressed hERG current by about 13% in hERG transfected HEK293 cells at 1 µM (>1000 times the estimated clinical free Cmax of lactone). The No Observable Effect Level (NOEL) of 0.3 μM is equivalent to circa 300 times the estimated clinical free Cmax of lactone.
No significant ECG abnormalities were noted in dogs in the PO and IV cardiovascular safety studies, nor in any of the repeat dose toxicity studies conducted in dogs or monkeys. Neither pitavastatin nor its lactone metabolite caused QT prolongation at 4 mg or at 16 mg in clinical studies.
https://www.tga.gov.au/sites/default/files/auspar-pitavastatin-130902.docx
I don’t think there is any supplement that will be better.
Just add enough omega3, fibers and physical activity to your Mediterranean diet. These three are safest, most studied and probably with most benefits in healthspan and longevity.
2 Likes
You’re not so interested in berberine anymore, lol?
I don’t think this will decrease apoB to 20-30 mg/dl.
And I don’t eat a mediterranean diet although I have tried to eat more of those foods in my diet.
This paper agreed with you
2 Likes
Berberine case report with long QT syndrome, together with hemp oil inhibitors:
We report the case of acquired long QT syndrome with torsades de pointes secondary to hemp oil and berberine supplements.
Yeah I’m probably skipping berberine.
When it comes to not falling over and dropping dead suddenly, pharma with all the safety data is much more preferable. Can’t trust a random supplement that doesn’t have a lot of research on safety.
3 Likes
Possibly you have too much of something? Like a heavy metal or Iron. This just happened to me.
2 Likes
Could BA/EZE + the lowest rosuvastatin (5 mg?) do the job? (as rosuvastatin seems to be the “safest” one)
2 Likes
Niacin in large doses increases the risk of diabetes. Pantethine should work well, I’m currently testing it (With Ezetimibe + low dose Rosuvastatin EOD)
2 Likes
Good point. I’ve just looked at things which help this: sauna, zinc, magnesium, vit c &e. Is there anything else?
1 Like
Vitamin E is not recommended as a supplement due to a link to cancer. The others should be fine or at least harmless.
3 Likes
It would be better with atorvastatin 10 mg, as compared to rosuvastatin 5 mg in RCT it has lower diabetes risk and cataract surgery:
The rosuvastatin group had a higher incidence of new onset diabetes mellitus requiring initiation of antidiabetics (7.2% v 5.3%; hazard ratio 1.39, 95% confidence interval 1.03 to 1.87; P=0.03) and cataract surgery (2.5% v 1.5%; 1.66, 1.07 to 2.58; P=0.02). Other safety endpoints did not differ between the two groups.
Atorvastatin is also a very popular drug on google trends, and it increased in popularity at the same time it became generic:
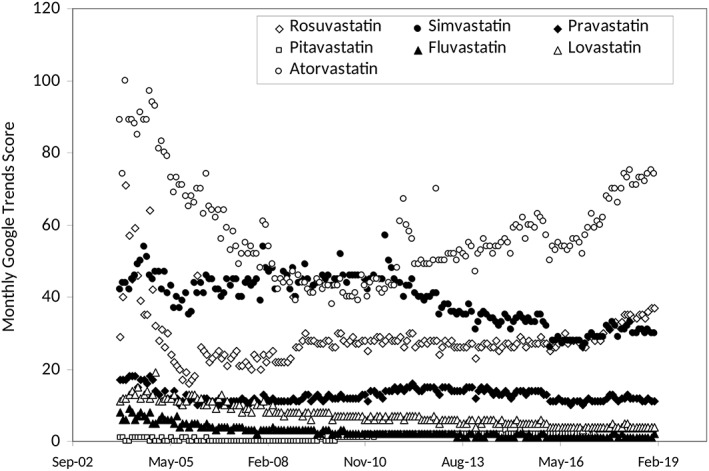
Statins popularity: A global picture 2019
I am quite certain there is no difference between statins based on lipophilic vs. hydrophilic status, they all cross the BBB according to Thomas Dayspring and it was really a marketing term and there is probably no clinically relevant difference in hepatoselectivity etc, with same side effects, only useful in as far different metabolism for drug-drug interactions maybe or RCT evidence. I did say earlier there was a difference, but it was regarding more vs. less hepatoselectivity. I have seen a recent study showing all statins cross the brain barrier confirming what he said, but I can’t find it. I think it was a review on statins and dementia or alzh.
Based on secondary outcomes in RCT’s, statins have either a neutral or positive effect on dementia including vascular dementia and no difference between hydrophilic/lipophilic statins according to Peter Attia based on clinical trials he reviewed in a recent premium article on statins I think.
There is speculation based on association studies long ago on serum desmosterol being associated with AD and mild cognitive impairment. Serum desmosterol is highly correlated with spinal fluid desmosterol. It is a marker of synthesis of cholesterol.
All statins cross the BBB and decrease synthesis of cholesterol. However, most cholesterol is already made in childhood and there is little synthesis in adulthood. Serum LDL etc does not enter the brain: https://twitter.com/Drlipid/status/1755985081900900367
So if anything if I can speculate since we are speculating based on association studies, those who genetically have a tendency to overproduce cholesterol (LDL, apoB?) might’ve already made a lot of brain cholesterol during the stages of life where a lot is produced, with the long half-life of 5 years. Suppressing synthesis a bit might have less of an effect if so.
I don’t either know how it affects all cause dementia in apoE4 carriers, and not many studies stratify on apoE4 status. Either way what we know with most likelihood is that statins have a neutral or positive effect on all dementia based on secondary outcomes. And then you can ride the speculation train either direction. One option is to not take statins and focus on drugs that do not apparently cross the BBB like PCSK9i, and those that don’t for sure like ezetimibe, bempedoic acid. PCSK9i, Bempedoic acid and Ezetimibe, would be most warranted if serum desmosterol decreases as it’s based on this hypothesis.
At the moment I would probably say that PCSK9 inhibitors, Bempedoic Acid and Ezetimibe is better. But that statins are pretty good as well. They all lower apoB which is most important. If money doesn’t make a difference, I don’t know if statins would be preferred to be used. It could be argued for, based on apoE4 status / family history of dementia, serum desmosterol levels, because of the amount of data that exists for them and maybe they make a different in the brain if someone is overproducing cholesterol there (vascular dementia?) (depression?) (inflammation?).
Edit: But it could be worthwhile anyway to use rosuvastatin… different metabolism allows for use with grapefruit juice, it is more potent, maybe the hydrophilic nature of it make some difference.
2 Likes
I believe you are overthinking the finer details.
Of course, it’s optimizing on the margin, lowering apoB is the goal.
“Never forget apoB is the goal not sterol levels per se. …”
https://twitter.com/Drlipid/status/1524919043727163396
2 Likes
As I said before, these studies tend not to include the second most common and fastest-growing neurodegenerative disease: Parkinson’s disease (and related Parkinson’s dementia). I emailed Brad Stanfield about that, suggesting a video “Statins and PD” similar to his recent one about dementia, he quickly answered: “Thanks Antoine for the support and video suggestion” ![]() .
.
Also: how are these trials designed? Let’s look at this 2008 trial of rosuvastatin:
Exclusion criteria were […] or another medical condition that might compromise safety or the successful completion of the study.
Such an exclusion criterion is not surprising. But would MCI or PD be considered such a condition? A few months or years is rarely enough to see a negative cognitive impact of a drug, with the exception of populations at risk such as people with MCI. Then:
All potentially eligible subjects underwent a 4-week run-in phase during which they received placebo. The purpose of this phase was to identify a group of willing and eligible participants who demonstrated good compliance (defined as the taking of more than 80% of all study tablets) during that interval. Only subjects who successfully completed the run-in phase were enrolled.
So basically, the trial was run only among statin-tolerant people. Are all statin trials designed like this? Per this source, “50% of patients prescribed a statin will cease therapy within the next 18 months”. Do statin RCTs also show a high non-adherence rate at 18 months? If not, then the population of these trials might be different, or they might exclude non-tolerant people as above. Also: how do they account for non-adherence in these trials? Could it be that statins have a negative impact on cognition only on some statin-intolerant people and that these people are somehow excluded from these trials or that they tend to quickly abandon statins after starting them?
1 Like
No, it was to select those who would be compliant, they only gave placebo.
I don’t think so. I think it’s a few percentage points difference.
Treatment compliance
Of the eight trials that reported treatment compliance there was no difference between the two groups (Analysis 4.1). In the statin group 77% participants and 70% in the placebo group complied with treatment; RR 1.08 (0.98 to 1.18).
I haven’t read this study but I think it’s likely to be true:
2 Likes
By the way, I like Dr. Lipid as well, last month he shared this recent paper: https://twitter.com/Drlipid/status/1745458968603037884
The paper, Alzheimer’s disease risk reduction in clinical practice: a priority in the emerging field of preventive neurology, is well worth a read. On statins, it concludes: “Although high LDL-C has been linked to increased AD risk and statin use has been linked to decreased AD risk, without large prospective studies, the target lipid level for optimal AD risk reduction remains unknown.”
2 Likes
Damned, I’m really tired this morning… Thanks for catching this, so my concerns are unfounded on statin tolerance and treatment adherence. The only potential issue is exclusion of those most at risk but it’s OK I think.
2 Likes
I wonder how compliant people are for drugs in general. I think I have heard something similar for drugs treating blood pressure. And why that is the case.
edit: It happens. It depends on your prior, I think the large studies are well run so I assume they are not extremely flawed. ![]() But JUPITER has some criticism I took up somewhere else…
But JUPITER has some criticism I took up somewhere else…
2 Likes
I also think the studies are well RUN, but I know (from friends in pharma) that they are designed to show a positive effect and that exclusion criteria and the choice of recruitment centers are the best way to improve your odds of success.
(and on drug compliance: yes. we discovered that our grandma was prescribed antihypertensive drugs a few months ago but never took them because she didn’t want to bother…)
2 Likes