Is the Nestle/Solgar version not available in the UK?
1 Like
Does anyone know any way to test these levels - either via blood spot or normal blood testing somewhere?
1 Like
I just used Table 1 here. 25/12.3*60 = ~120. I mentioned ChatGPT about the one-week on/one-week off schedule, as I thought that because one week of a mouse is like 4 months of a human, we would need longer periods of pause. But ChatGPT said no (without much reasoning).
Safety: no idea at all. We have almost zero long-term data on UA. Maybe we have long-term data on pomegranate juice consumption, or pomegranate supplement use.
Nothing on their website: https://solgar.co.uk
I emailed them.
Still good to know for Americans that Mitopure is a bit cheaper on Nestle’s website: https://www.nestlenutritionstore.com/shop-by-categories/adults/cellular-nutrition.html
Also, for anyone interested: BREW30 gives 30% discount on Mitopure Softgels | Timeline Nutrition (not promoting it, just saying)…
4 Likes
I don’t know if this is a good journal or team but this paper argues that Urolithin A + green tea extract EGCG is even better than UA alone.
EDIT: the same authors made the same claim one year earlier in a way better journal (Pharmacological Research): Mitophagy enhancers against phosphorylated Tau-induced mitochondrial and synaptic toxicities in Alzheimer disease 2021
We recently optimized the doses of mitophagy enhancers urolithin A, actinonin, tomatidine, nicotinamide riboside in immortalized mouse primary hippocampal (HT22) neurons. […] Further, urolithin A showed strongest protective effects among all enhancers tested in AD. Our combination treatments of urolithin A + EGCG, addition to urolithin A and EGCG individual treatment revealed that combination treatments approach is even stronger than urolithin A treatment. Based on these findings, we cautiously propose that mitophagy enhancers are promising therapeutic drugs to treat mitophagy in patients with AD.
6 Likes
As UA inhibits mTOR, is it better to cycle it? How often? Is it better to take it in the morning? In the evening? With or without food? ![]()
In terms of half-life, I found this:
- “The washout period was considered effective and not to have influenced the results during the crossover design, as UA has a half-life of ~24 h with elimination following a single oral dose occurring after between 3 and 4 days” (Direct supplementation with Urolithin A overcomes limitations of dietary exposure and gut microbiome variability in healthy adults to achieve consistent levels across the population 2021)
- “It showed a relatively long-half life (t1/2 = 17–22 hours), most likely due to an active enterohepatic recirculation.” (Impact of the Natural Compound Urolithin A on Health, Disease, and Aging 2021)
- “The biphasic kinetics was shown for metabolites, probably due to enterohepatic circulation. The half-life (t1/2) ranged from 17 to 22 hours for the parent compound and urolithin glucuronide, while it was slightly longer (25-58 hours) for urolithin A sulfate.” (Ellagic Acid-Derived Urolithins as Modulators of Oxidative Stress 2020)
(to compare: “The half-life of rapamycin is 58–63 hours (~ 3 days).”)
In this mice study they use 2.5 mg/kg UA (that’s 10x less than in the 2023 Buck Institute paper that showed life extension) + 25 mg/kg green tea extract EGCG. The UA+EGCG combination seems about 15% more potent than UA alone looking at figures and tables (guesstimate). Interestingly, they still cycled UA even with this low dose: “3 times per week for 4 months.” And they still had good results.
If my above reasoning is correct (maintenance dose of 90 Mitopure pills per year), then with EGCG, you can instead use only 77 pills. You can probably even decrease to 60 pills/y, meaning one Mitopure Softgels sachet ($125 to which you need to add the cost of EGCG). Of course, we don’t have evidence yet evidence this dosing regimen in human adults would have any benefits.
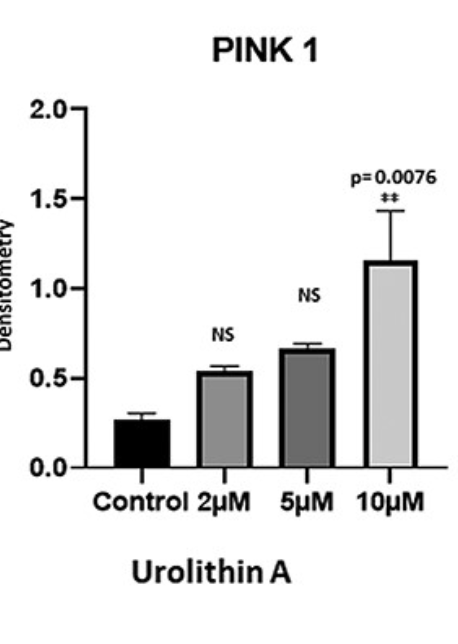
I don’t know how to make sense of the 10x difference in terms of dose between the two studies. The authors of the 2022 paper (that used the lowest 2.5 mg/kg dose) wrote: “We recently optimized doses of mitophagy enhancers urolithin A, actinonin, tomatidine and nicotinamide riboside in HT22 cells” and they cite this paper: Protective effects of mitophagy enhancers against amyloid beta-induced mitochondrial and synaptic toxicities in Alzheimer disease 2021. They only tested 0, 2, 5, and 10 μM of UA directly on cells, and there was a quasi-linear dose-response relationship. Would 100 μM be even better? ![]()
In the Mitopure study on middle-aged humans, they compared 500 mg (the commercial Mitopure dose) to 1,000 mg, and found that 1,000 mg was better.
In this 2023 study (by Amazentis) they even “supplemented with UA oral targeting 50mg/kg/day” on mice (Study 2)! Urolithin A induces cardioprotection and enhanced mitochondrial quality during natural aging and heart failure (preprint)
Anyway, I bought one Mitopure pack (60 pills). I’ll see what I do. I’m hesitating between (with or without EGCG in each case, TBD):
- Following the recommended Mitopure regimen (500 mg/d = 2 pills) for a month then see or,
- 1 pill (250 mg) every other day, one week on, one week off,
- 2 pills (500 mg) per week.
Feedback welcome ![]()
Also, Solgar UK answered my email regarding Mitopure:
Unfortunately we don’t sell this product here in the UK. It sells well abroad but there isn’t enough demand for it in this country at the moment.
A lot of our products are available to buy from reputable online retailers such as Amazon, or from specialist import/export retailers.
If other UK residents email them we could maybe convince them that there’s enough demand. poke @Walter_Brown
3 Likes
Interesting. Some lucky people have the gut bugs to make urolithin A in their guts. Are they getting an mTOR down regulation 24/7/365? If material (in impact size), that would show up somewhere I’d think.
Is urolithin A for people with mitochondrial problems (trying to recover) or people looking for better than normal mitochondrial function or people who don’t want to exercise but have healthy mitochondria?
1 Like
To make UA I understand that you need 1/ a healthy gut and 2/ a diet rich in pro UA food such as pomegranate juice.
I guess no one knows yet what UA is for but researchers seem to think that it could be both for people with severe mitochondrial dysfunction (due to old age, Parkinson’s, Alzheimer’s, etc.) or for “healthy” mitochondrias but who want to enhance them (from “normal” to “optimal”).
3 Likes
OK, now I know: the lowest dose (2.5 mg/kg) was administered via intraperitoneal injection: “Urolithin A group: hAbKI mice were administered with urolithin A (2.5 mg/kg body weight) (i.p.), optimized in our lab, 3 times per week for 4 months” whereas the larger doses (25 mg/kg or 50 mg/kg) were administered orally either mixed with food or given via gavage in liquid form.
And according to this paper:
therapeutic potential of UA is constrained by poor bioavailability
So this can explain the 10x difference in dosing between oral and IP UA. This solves the dose question in mice at least. The dosing schedule question is still open: pulsing? how often?
This study (already cited) might also answer your question @Joseph_Lavelle:
Density and number of mitochondrial cristae was markedly decreased with age, as evidenced by the loss of strict parallel position (Fig. 2A and 2B). UA intervention rescued the age-dependent decline in cristae volume density to levels compared to those observed in young animals (Fig. 2A-B). Interestingly, mitochondrial cristae were more circular with age, while UA administration to old animals reverted such increase (Fig. 2C). Regarding mitochondrial morphology, mitochondria were smaller in old compared to young animals, an effect rescued by UA administration (Fig 2D). No differences in mitochondrial volume density and mitochondrial number were observed with UA in either young or old mice (Suppl. Fig. 2A and 2B). These results indicate that age-associated alteration in heart mitochondrial morphology and ultrastructure are reverted by 2 months of UA supplementation, while neither aging nor UA affected mitochondrial content.
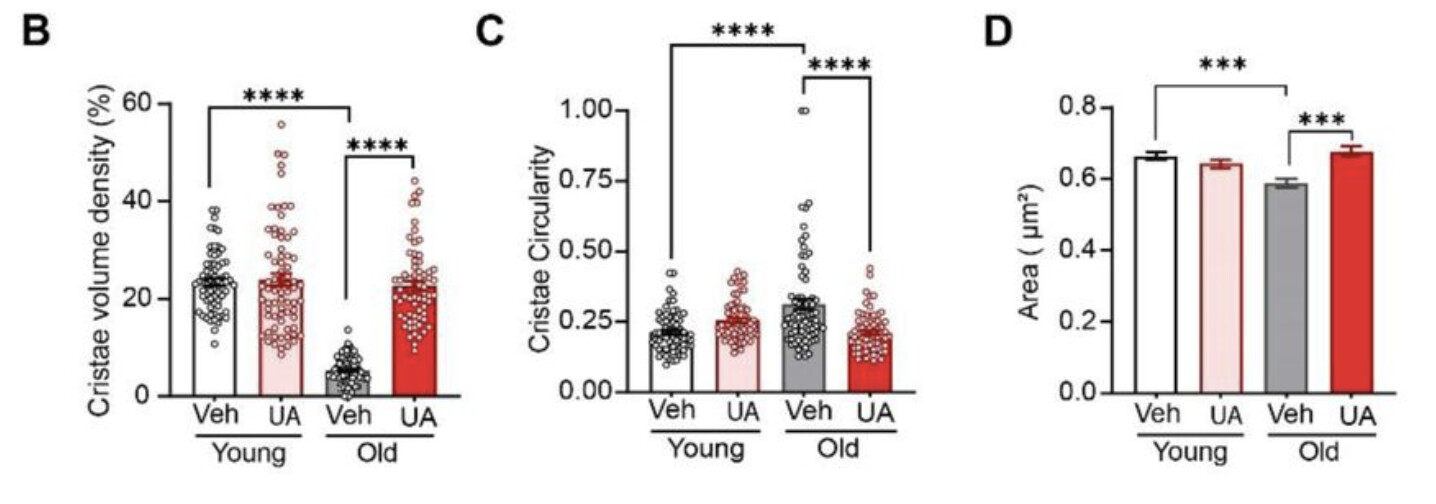
So it looks like among young mice, 2 months of UA supplementation has no effect whereas it reverses age-associated alterations in old mice. So can it be useful in healthy individuals? I don’t know. What are ways to measure mitochondrial health? (volume density as they did?)
3 Likes
@adssx This is excellent information. Thank you. Do you still think a short term, periodic use of urolitin a (500mg/ day or every other day) for a month would work in an older person like an older mouse?
1 Like
I don’t know.
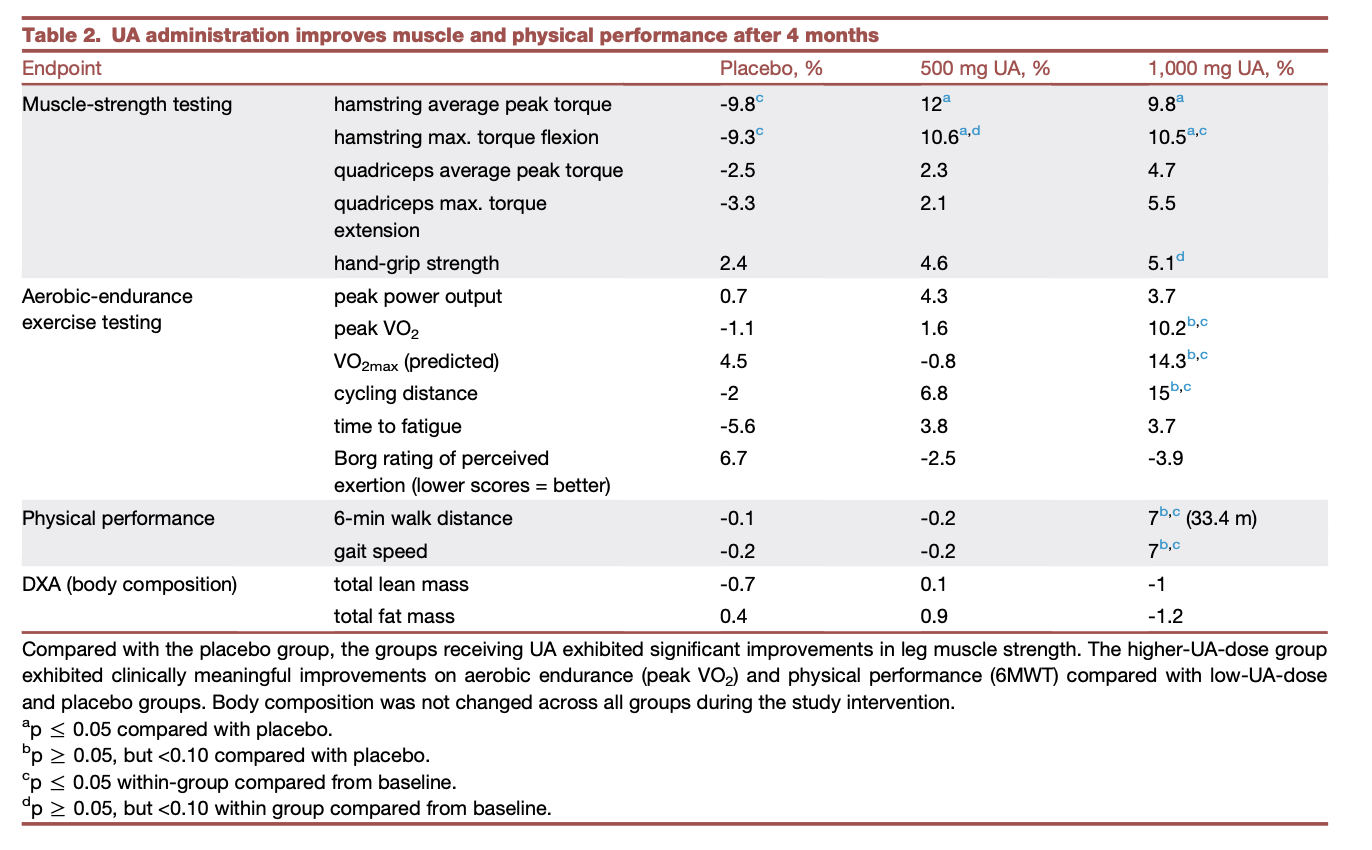
The most related paper we have is this one by the Mitopure team: Urolithin A improves muscle strength, exercise performance, and biomarkers of mitochondrial health in a randomized trial in middle-aged adults 2022
The study population consisted of untrained adults between 40 and 64 years of age. In addition, subjects were screened on the criteria of being overweight and having low physical endurance (i.e., maximum oxygen consumption [VO2max] <35 kg/mL/min). A 4-month intervention period was selected as the minimal time period to start detecting an impact on physical-performance- and muscle-functionrelated study endpoints based on guidelines and recommendations of expert groups on clinical trials focused on muscle function.
Even after 4 months in this unhealthy population, only the highest dose showed (very) significant improvements (+14.3% VO2max!):
So I wonder:
- Do you need long-term treatment to see the effects? (the mice studies were done for 2 months, meaning years for humans)
- Do you need even higher doses?
- Would pulsing increase the effects?
Also, I find it weird that their 2021 study (pomegranate juice vs Mitopure) found that:
Age had no impact on UA generation or absorption as well as UA producer status as levels were consistent across the different age groups of young, middle-aged, and elderly (Fig. 5D) both with direct UA supplementation and following PJ intake.
2 Likes
Interesting. I think I’m going to just keep watching this and focus on exercise, rapa, and protein cycling. I’m having good success with GG in repairing damage done / issues caused by statins so I don’t have an urgent need.
2 Likes
What’s GG? ![]()
1 Like
Details on GG here
2 Likes
Thanks.
Small numbers but interesting qualitative feedback here: https://www.reddit.com/r/Nootropics/comments/13wk8h7/anyone_has_experience_with_urolithin_a_mitopure/
It looks like Mitopure can drain your energy, at least at the beginning, and cause some insomnia. It could be another reason to cycle it.
2 Likes
It would be interesting to see the longevity information for those individuals who naturally produce high levels of UA. These individuals have been out there for generations. Sadly, it doesn’t seem like this supplement will push us past the 120 yo age barrier.
1 Like
I don’t think we have any commercially available supplement or medicine that would do that yet?
Have you looked if there is any Mendelian Randomization instrumentation on this? That could help answer your first question.
1 Like
I haven’t been able to spend more time on it yet.
My current rough concept / prelim thinking / is to perhaps do 3-4 sessions a year (similar to my fasting goals, but spread out roughly midway between the fasting times). And perhaps do the full “marketed” dose each day during a 4 week period to do some housekeeping of mitophagy followed by mitochondrial biogenesis. And then the rest (and majority of the time) not be on any Mitopure at all.
But this is just an idea I’m playing around with - I have not settled on it yet.
3 Likes
Thanks, it’s also my best guess for now. Receiving my Mitopure on Monday, I’ll probably follow the 4-w mitochondrial “housekeeping” and then see…
Another great article about UA: Mitophagy curtails cytosolic mtDNA-dependent activation of cGAS/STING inflammation during aging 2024
In old mice, pharmacological induction of mitophagy with urolithin A attenuates cGAS/STING activation and ameliorates deterioration of neurological function.
We conducted neurophysiological, behavioral, and retinal immunohistochemical and transcriptomic analyses in young (6 months) and old (22 months) mice injected intraperitoneally with UA (2.3 mg/kg) or vehicle daily for 8 weeks
Mass spectrometry (UPLC-ESI-QTOF-MS) of perfused brains, and plasma samples as positive controls, showed that free UA crossed the blood-brain barrier and reached the central nervous system.
UA treatment significantly increased mitophagy in the neuroretina (Fig. 4b) and RPE (Fig. 4c) of young and old mice, albeit to a lesser extent in the latter. Hindlimb clasping score, used as a readout of general neurological function, was significantly lower in old UA-treated mice versus vehicle-treated counterparts (Fig. 4d). Old mice treated with UA treatment also showed improved recognition memory […] UA-treated old mice showed improved scotopic (dark) vision […] Immunohistochemistry indicated that UA ameliorated CtBP2+mGluR6+ synaptic integrity in old mice (Fig. 4h), further suggesting that UA promotes the preservation of visual function during aging. UA also decreased lipid peroxidation-derived 4-HNE+ aggregates (Fig. 4i), indicating that improved mitochondria quality control may also reduce oxidative stress in the aging retina.”
3 Likes
Cool. Are there any tests you will do before and after?
2 Likes