To validate this score, PROSPR will run the first Phase 3 clinical trial targeting aging in people not yet diagnosed with a specific disease, evaluating three drug targets already approved by the FDA for other conditions: rapamycin, which acts on cellular pathways linked to aging; newer obesity and diabetes medications known as GLP-1 agonists; and diabetes drugs called SGLT-2 inhibitors that also benefit the heart and kidneys.
And as a second step
The program will then test whether novel compounds designed specifically to target aging biology can be evaluated the same way.
And can provide a valuable toolkit for biohackers too:
If the score proves accurate, it won’t just be a research tool; individuals could use a home testing kit to determine whether their lifestyle choices or treatments are actually making a difference. Our goal is to have that testing kit cost less than $100 by 2031.
Seems like the near term, first trial with rapa, dapa and sema (not the new novel drug candidates like the new Cambrian mTOR one) is as follows
The VITAL-H Trial Overview
Backed by up to $38 million in ARPA-H funding, UT Health San Antonio is launching the first nationwide clinical study focused on healthy longevity. Instead of targeting a specific disease, the trial aims to see if midlife interventions can delay age-related physical and cognitive decline in generally healthy adults aged 60 to 65.
To do this, they are repurposing three FDA-approved medications that have shown strong preclinical and early human data for targeting the biological hallmarks of aging:
• Rapamycin (mTOR inhibitor)
• Dapagliflozin (SGLT2 inhibitor)
• Semaglutide (GLP-1 receptor agonist)
This effort targets generally healthy adults ~60–65, with endpoints framed around Intrinsic Capacity plus decentralized/wearable measurement
A Stanford/Buck/Methuselah-linked team (“THRIVE”) is building an FDA-grade Intrinsic Capacity score (PROSPR-IC) intended to predict long-term outcomes and enable shorter trials.
A Columbia-led effort (“FAST”) will mine completed trials/biospecimens to find biomarkers that respond to interventions—including rapamycin, SGLT-2 inhibitors, GLP-1 agonists—to support PROSPR’s shorter trial model.
Yes, this is great news. Great drug selection. It seems like they’re listening to the scientific community when they selected these 3. Honestly, though, I would have added a lipid-lowering medication just to help prevent CVD deaths, which will skew the results due to death by heart attack/stroke. Dapagliflozin will help, but add a direct lipid-lowering med like BA and Ezetimibe, and I think the results will be better!
My guess it that the PM is interested in aging and not just healthspan and since the world knows that CVD is importantly and largely how to treat it that would lead to less valuable learnings?
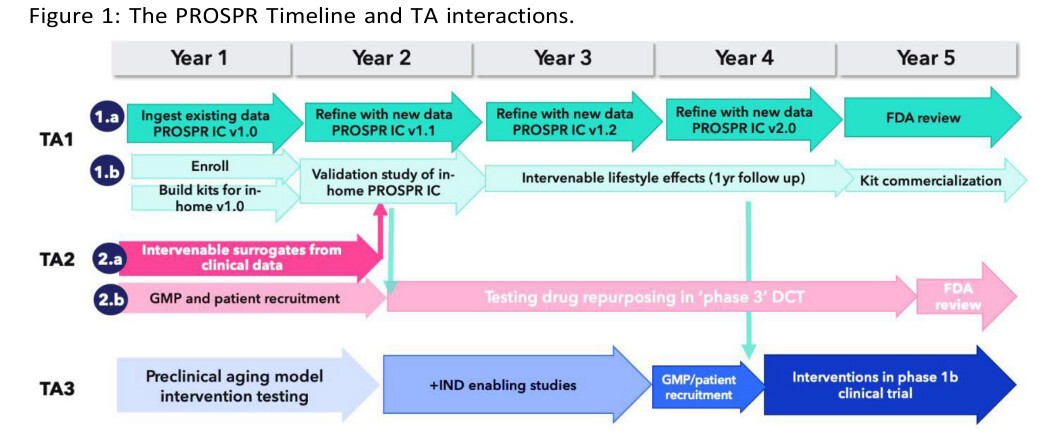
Stanford University in Palo Alto, CA will harmonize the vast existing health datasets collected by multiple institutions to generate a healthspan score (PROSPR-IC score). They will test the accuracy and intervenability of this score in a 1-year lifestyle intervention, which will be supported by an in-home digital health assessment technology they develop.
The University of Texas Health Science Center at San Antonio in San Antonio, TX will establish a regulatory path for testing the efficacy of therapeutics for aging by conducting a phase 3 hybrid trial to repurpose three FDA-approved drugs: SGLT2 inhibitor, rapamycin, and semaglutide.
Columbia University Mailman School of Public Health in New York, NY, aims to identify biomarkers that are responsive to interventions that improve aging outcomes in humans by performing combined analysis of multiple, previously performed intervention trials.
Apollo Alpha in St. Petersburg, FL will test whether an orally bioavailable compound that crosses the blood–brain barrier and targets energy homeostasis, lipid metabolism, and inflammation will improve aging outcomes.
Cambrian BioPharma in New York, NY will test whether a daily, oral, novel rapamycin analog will improve aging outcomes.
Linnaeus Therapeutics in Haddonfield, NJ, will test whether a compound with an established safety profile, demonstrated cardiometabolic benefits, and once-daily dosing improves aging outcomes.
The University of Rochester in Rochester, NY, will evaluate whether a compound with an established human safety profile and high relative potency within its class, can improve aging-related outcomes.
The problem is that whenever you are talking about longevity, you have to address the 800 lb gorilla of CVD which kills about 1/3 of the population. If a large number of participants die early due to CVD, you won’t be able to get a good read on how well these other interventions extend longevity unless you throw out any results that are impacted by CVD and arteriosclerosis, but I’m not sure how you’d do that.
However, it’s a lot better than nothing and I am sure there will be some positive results. So, it’s a win.
Semaglutide shows very promising results for CVD.
I wish they chose Tirzepatide instead of Semaglutide. The only reason Semaglutide is a better choice is that it isn’t on patent anymore as far as I am aware, and it is quite affordable.
There’s also the problem with Rapamycin: it increases lipid levels and blood sugar in some individuals (my ApoB went up 33%), and if they are using that as an aging biomarker, then Rapamycin would look like a lifespan-shortening drug. Only after taking BA + EZ + statin did my ApoB drop from 120 to 58. So my ApoB went from 90 (nothing) to 120 (Rapa) to 58 (Lipid control).
I’m not sure if the researchers will be aware of or control for these side effects. They really should consult with us for some firsthand experiences about potential pitfalls/complications. @Rapadmin
It’s not powered to detect differences in CVD rates that’s why they use IC and it’s healthy older adults. ApoB is a possible side effect that should be monitored and addressed of course.
WOW, so much for new admin cutting funding for research. Clearly there is a much more proactive and focused approach to healthy aging and longevity than administrations in the past. Now that the attention has turned to treating aging as a disease great things should unfold in next 3-5 years IMO.
I think Marty Makary is trying to do the right things. Federal spending on health is huge and inevitably wasteful regardless of who’s in charge. Some babies will get thrown out with the bath water, but some good work will begin.
I’d even go as far as to say that without lipid-lowering medication this whole study is doomed to begin with. Might aswell inject someone with the Yamanaka factors then cut their head off and declare the Yamanaka factors don’t work.
Although I am glad to see a Phase 3 trial starting on Longevity I would like to issue a warning about the use of Semaglutide. I am the moderator of a world-wide forum on a somewhat rare eye condition called NAION. It usually happens to people over 50 while they sleep and they awake to find permanently distorted vision in one eye. In the past year we have had several new members who took Semaglutide who have developed this disease in a completely different mode. It has come on them slowly over a period of weeks. Age does not seem to be involved. There are now several class action lawsuits in the US, GB and Europe that I am aware of against the manufacturer(s). If you want to start use of Semaglutide I strongly suggest you visit a competent Neuro Opthamologist to see if you have a genetic condition known as “disc at risk” in either eye as this is the best known precursor for NAION. The other common contributor seems to be sleep apnea. If you have either of these conditions you would be smart to not use Semaglutide.