The Peptides Quietly Accelerating Aging with Dr Valter Longo, interviewed by Simon Hill

Dr. Valter Longo, a longevity researcher with 30+ years studying the growth hormone (GH) / IGF-1 / TOR axis, delivers a pointed critique of the current peptide and GLP-1 craze, arguing that consumers are catastrophically over-weighting short-term cosmetic and performance gains while ignoring decades of convergent evidence that elevating GH/IGF-1 signaling shortens life and accelerates disease. The core thesis: the same biological axis that produces visible short-term benefits (muscle gain, fat loss, “feeling reinvigorated”) is the most well-validated pro-aging pathway in biology, demonstrated across yeast, worms, flies, mice, and humans.
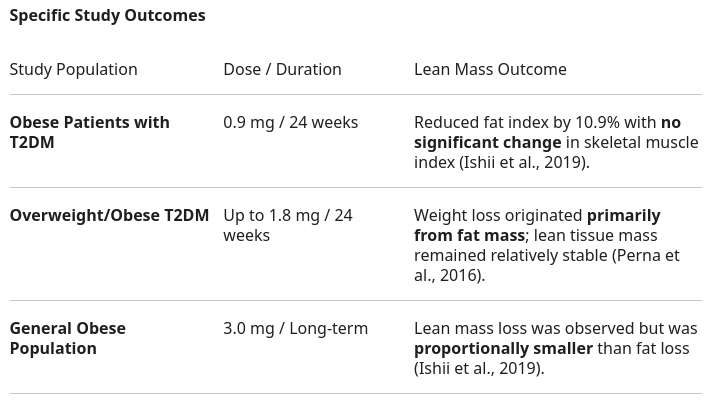
On GLP-1 receptor agonists, Longo concedes a real ~10% mortality reduction in obese populations but argues this is dwarfed by the ~25% reduction available from a Mediterranean dietary pattern delivered by competent professionals. He cites long-term data showing 92% discontinuation by year three, rapid weight regain post-cessation (due to endogenous GLP-1 suppression analogous to exogenous testosterone suppressing HPG axis), and net loss of lean body mass over multi-year follow-up.
On GH secretagogues (ipamorelin, tesamorelin, CJC-1295, MK-677-class compounds), Longo is categorical: these are not a regulatory gray-zone experiment — the underlying biology has 100 years of research showing the inverse direction is what extends life. Laron-syndrome cohorts (GH-receptor deficient), Snell, Ames, and Laron dwarf mice all show ~40% lifespan extension and dramatic reductions in cancer and diabetes incidence. Acromegalic patients (the natural human equivalent of chronic GH excess) die early from cardiovascular disease and metabolic dysfunction; FDA-approved drugs exist specifically to suppress GH/IGF-1 in this population.
Longo’s positive program centers on the Fasting-Mimicking Diet (FMD): a 5-day, ~770–1100 kcal/day, plant-based, low-protein, relatively high-fat protocol cycled 3–4×/year. Published trials show no lean-mass loss, ~2.5 years reduction in biological age (PhenoAge/BioAge), proteinuria reversal in CKD, and benefits in Crohn’s and ulcerative colitis. He recommends an everyday “longevity diet”: pesco-vegan, ~0.8 g/kg protein, plant-dominant amino acid profile, ~50% carbohydrates from non-starchy sources, with explicit warnings against low-carb diets, animal-protein loading, and any peptide that pushes IGF-1 above ~200 ng/mL.
Adopt a low-protein, plant-forward dietary pattern. Target 0.8 g protein/kg body weight from a 2:1 plant:animal ratio (or higher plant share), with fish 2–3×/week. Convergent evidence from PREDIMED, Lancet Public Health carbohydrate cohort, Harvard nurses/health-professionals follow-up, and Blue Zone epidemiology. Estruch et al., NEJM 2018 | Seidelmann et al., Lancet PH 2018
Twelve-hour time-restricted eating window. Compress all food intake into a 12-hour window daily. Supported by RCT and mechanistic data. Source unverified in live search.
Resistance training is the dominant lever for lean mass. Protein loading above 1.2 g/kg adds marginal hypertrophy in the absence of training; training without adequate protein still fails. Prioritize the training stimulus.
If overweight/obese and prior structured dietary intervention has failed, GLP-1 receptor agonists are reasonable — but only as a bridge inside a competent clinical program addressing root-cause behavior change, paired with resistance training to limit lean-mass loss. Wilding et al., NEJM 2021
Fasting-Mimicking Diet, 5-day cycles, 3–4×/year for healthy adults; monthly initially for metabolic disease or autoimmune indications, tapering as markers improve. Strong mechanistic and emerging clinical data, large safety database (~1M users, mostly Grade ≤2 events). Coordinate with physician if on insulin, hypoglycemics, or for any active disease state. Wei et al., Sci Transl Med 2017 | Brandhorst et al., Nat Commun 2024
Target circulating IGF-1 in the 120–160 ng/mL range via dietary protein quantity and source manipulation. Recheck annually. Source unverified in live search.
Combination FMD + short-acting GLP-1 (proposed but not yet trialed) — Longo signaled interest in testing whether a 2–3 day GLP-1 oral burst can blunt FMD hunger without inducing lean-mass loss. Currently hypothesis-stage; do not self-experiment.
GH secretagogues (ipamorelin, tesamorelin off-label, CJC-1295, MK-677, sermorelin) for longevity or anti-aging. Mechanism directly opposes every validated longevity signal in biology. Human comparator (acromegaly) shows accelerated cardiovascular disease, insulin resistance, and shortened lifespan. No Phase III longevity RCT exists; no chronic safety data in healthy users. Safety Data Absent — Evidence Direction Adverse.
Unregulated peptides sourced from foreign suppliers and self-reconstituted with bacteriostatic water. Identity, purity, endotoxin contamination, and dose are all unknown. Sterility breaches and immunogenic reactions are documented risks. Safety Data Absent.
Exogenous human growth hormone for anti-aging in adults without documented deficiency. Same axis-activation problem as secretagogues; off-label use is illegal in the US for anti-aging indications. Evidence Direction Adverse.
Low-carb / ketogenic diets high in animal protein and saturated fat for longevity. Short-term metabolic markers may improve; long-term cohort data show elevated all-cause and cardiovascular mortality. Seidelmann et al., Lancet Public Health 2018
High-protein diets (>1.5 g/kg) dominated by animal sources when chronic IGF-1 elevation is undesired. Levine et al., Cell Metabolism 2014
Bottom-line clinical posture: The visible short-term effects of GH-axis activation (muscle, vitality, fat loss) are real and uncontested — and so were the short-term effects of cigarettes on body weight. The translational question is not whether these compounds do something, but whether the something they do is the same direction that 100 years of comparative biology says you want to move. The convergent answer across yeast, invertebrates, three independent dwarf mouse strains, the Laron Ecuadorian cohort, and acromegalic patients is unanimous and points the opposite way.
This seems consistent with much that I have read lately about the issue of body recomposition – even if you don’t experience fat gain after quitting. Also consistent with personal experience – even after very short, low dose, lost muscle that has taken months of work to even partially regain.
Cher reportedly said: “If a great body came in a bottle, everyone would have one.”
I listened to this interview when it first came out and it’s pretty interesting toward the end, like the last 20 minutes or so about FMD and yamanaka factors repairing tissue and organ damage. One unfortunate element of the interview is that Longo makes slips of the tongue several times, where he says something while meaning the opposite - if you are very familiar with the subject matter, you will catch that, but if not, you might be misled and walk away with some wrong information.
Obvious, since FMD doesn’t lead to more than 15% weight loss, and it goes on for at most 1 week. There’s nothing special about GLP1 weight loss that makes it prone to lean mass loss. If you lose a lot of weight in a short period, you will lose muscle mass. Control the rate of weight loss and exercise.
This is actually much less useful than it seems. If you know anything about measuring igf1, you know that it is highly dependent on the machine model, reference range, and assay used. And this is why you ask for z-score, so you can compare levels across these variables. This range could mean anything. He should be talking about IGF1 z-score.
The 25% figure quoted is actually for relative risk reduction. The absolute risk reduction for FMD is actually closer to 1%. For comparison, in the LEADER trial, liragultide had an ARR of 1.3%. So these look about the same to me. Note that they had to re-publish PREDIMED due to flaws in the design of this study. See https://www.bmj.com/content/364/bmj.l341.long
Thank you. That is one of my pet peeves. So, many papers and articles use relative risk reduction as “clickbait” nonsense. I don’t give a damn about relative risk reduction. It often produces much larger, more “headline-worthy” numbers.
"A drug company might advertise that a pill “reduces the risk of a stroke by 50%.” That sounds life-changing. However, if the original risk was only 2 in 1,000 (0.2%) and it dropped to 1 in 1,000 (0.1%), the actual reduction is only 0.1%. "
presumably Rapamycin activates this Yamanaka-factor-driven reprogramming too?
The paper suggests it does it specifically states that the regenerative effects observed from the FMD are recapitulated by mTOR inhibition, suggesting that pharmacological mTOR inhibitors (like rapamycin) can trigger similar pathways to restore insulin generation?
That’s seems intuitively right but is there any evidence that low dose/slow weight loss from GLP1s results in a lower proportion of muscle loss? If there is then it seems a pretty important bit of information for potential users
There’s been some studies showing liraglutide is very good at retaining lean mass. The total weight loss it provides is also 2-10x less than the ones provided by the newer generations of GLP1 agonists.
If worried about lean muscle mass, keep in mind that apparent muscle mass reductions are due in part to less fat accumulating in the muscle, and thus the muscle losing some volume. This was verified by measuring by CT.
The skeletal muscle biomarkers, including muscle area, muscle attention, and IMAT area, showed interesting patterns in the various groups in the current study. As previously noted, muscle area decreased in the weight-loss group and increased in the weight-gain group. Muscle attenuation showed significant decreases in the intermediate-weight-change and weight-gain groups. Such decreases may indicate diminished muscle quality, presumably related to accumulation of intramuscular fat (i.e., myosteatosis). The decrease in muscle attenuation was particularly pronounced in the weight-gain group, consistent with the significant increase in the IMAT area in this group
In GLP-1 studies, a significant portion of “lean mass loss” actually comes from liver mass and other internal organs, which shrink as systemic inflammation and fat storage (steatosis) decrease.
The observed solid-organ findings also suggest favorable longitudinal changes in ectopic fat deposition associated with weight loss in patients with semaglutide use. For example, the weight-loss group showed a significant decrease in liver volume and significant increase in liver attenuation, consistent with decreased fat content. In contrast, the weight-gain group showed no significant changes in liver volume or liver attenuation.
https://www.ajronline.org/doi/10.2214/AJR.24.31805
This analysis says GLP-1RA treatment was associated with substantial reductions in fat mass and relatively modest declines in fat-free mass of approximately 2% to 3%. Measurement was made by BIA:
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2843518
Despite losing absolute muscle mass, relative strength often improves. For example, in STEP-1 Trial, participants on semaglutide lost lean mass, but their “power-to-weight ratio” and physical mobility scores actually increased because they were carrying significantly less fat mass. Studies tracking handgrip and knee extension strength show that these metrics remain stable or improve on GLP-1s.