I was also taking empagliflozin for most of that time (recently stopped in order to get hematocrit under control). I just started an ARB about 6 months ago (first irbesartan and now telmisartan 80mg QD). So the LVH reversed despite high testosterone (which I wasn’t even taking at baseline) significantly increased weight training and minimal cardio, all of which would have been expected to exacerbate LVH.
It looks like the combo of SGLT2I and ARB is an amazing 1-2 punch for LVH, but the hematocrit elevation from SGLT2I and testosterone should be taken very seriously. See my post in the SGLT2 thread on a new study.
I can’t tell you what you should do because that’s between you and your medical provider, but it’s a combination that seems to work well for a lot of people. Telmisartan helps control blood pressure, reduces risk of LVH, has other potential positive metabolic and health benefits, and even has a small effect on lowering hematocrit, all with a relatively low risk of side effects. My PCP had no problems prescribing it for me.
Only mentioning for younger males with some T, the bioregulator Testoluten has helped many and Ovagen for women, since their T comes from aromatased E in the ovaries (pre menopause), injected or topical as for men post menopause. No data on boron >= 10mg, but is popular. I buy oral bioregulators at biolongevitylabs.com. They have the faster acting injectable too. I do both for anti aging, loosely following Bill Lawrence’s bioregulator protocol; cycling each for a month in order: chronoluten, vesugen, pinealon, epitalon, ending on livagen (an epigentic flipper to cement the changes). Probably better as a thread in the bioregulators area.
My observations are that Licensure is a hindrance in treating the hardest autoimune, chronic cases. I’ve slowly found a group of unlicensed health coaches that built a concierge business model serving zoo animals to elite athletes to sports teams, well off cancer patients and in between. Some compounds are referred to by chriptic names some months out of a bio-lab. Sounds risky, but so is death and the Alopathic system of pushing $50k per dose but 1% absolute benefits is failing.
Bioregulators are 50-60 yr old from Russia. Recently higher quality mfgering, consistent content thus consistant efficacy has even licensed Functional practicioners to health coaches using injected (fast but short acting) through oral (slower but more permanent longer acting) bioregulators. This modality is similar to TCM, tradional Chinese Medicine in that; small changes daily sum up to large long term change.
Because no patents or $50k per dose is possible there will never be so called “quality studies”. The efficacy and practice is through hand me down learning amounst the practicioners and the inside circles of health groups that have subtle solications off youtube channels. I’m in a few peptide free groups on Skool. And one $200/mo one also on skool. My wife got in early with an inside circle with Nattaly Niddam, an early adopter, licensed, or was, then went Youtube’er and pay for inside circle coach. Niddam today has lost relavance IMHO.
Whats coming out of the labs into these inside circles is useful. Maybe you’ve read about yet another compound in our bodies that falls off in the leagues of Growth Hormone et al with testostorone, E, free_t3, etc. Its Klotho. My daily injection of klotho is on order. Mean time I tried a publicly purchasablee klotho off Biolongevitylabs.com, that also sells bioregulators, injected and oral.
I’m getting long winded… I’ve read amazing case studies of extremely sick folks being resusetated by skilld practioners with mainly life style, diet and bioregulators. Autoimune issues is an area bioregulators in the hands of a skilled practioner can be solved. Typically after a dozen Alopathic time and $$$ wasters.
Not really… my prostate is about the size of a walnut… 20 year old size… due to daily finesteride for 30 plus years.
Been on this dose of testosterone for 6 full years… everything checks out. Again testosterone is natural to the body… high normal… is still normal zone. So risk is less than that of high steroid abuse 1000 mg upwards.
Just got my PSA last week .93 not even 1.
Soooo. I think all good… family genetics no cancers or CVD.
I used TRT off and on for a few years, stayed in the 600-1000 range. T is below 300 when not on TRT. Have some BPH and PSA 2.5 so ok for 75 yrs. Just started Rapamycin so optimistic about prostate cancer chances. But still cautious. Been on Finasteride 2 years.
I had not heard of this as a risk factor so I checked on it.
Testosterone Levels and Cancer Risk
1. Claim: Testosterone therapy does not increase the incidence of prostate cancer in men without a prior history.
Evidence Level:Level B (Human Randomized Controlled Trial)
Verification: The TRAVERSE trial is the definitive, large-scale (n=5,246) study mandated by the FDA to assess this exact risk. It found no significant difference in prostate cancer incidence between the testosterone and placebo groups over a mean duration of 33 months.
Source: Lincoff, A. M., et al. “Cardiovascular Safety of Testosterone-Replacement Therapy.” The New England Journal of Medicine, 2023.
2. Claim: The “Saturation Model” indicates that prostate cancer growth is insensitive to testosterone concentrations above a low threshold (approx. 250 ng/dL).
Evidence Level:Level C (Review of Human Observational Studies & Mechanistic Data)
Verification: This model, proposed by Dr. Abraham Morgentaler, unifies clinical observations that while castration (low T) reduces prostate volume, supraphysiological T does not increase it further. It explains the lack of dose-response relationship in clinical trials.
Source: Morgentaler, A., & Traish, A. M. “Shifting the paradigm of testosterone and prostate cancer: the saturation model and the limits of androgen-dependent growth.” European Urology, 2009.
3. Claim: Low serum testosterone is associated with more aggressive (high-grade) prostate cancer.
Evidence Level:Level A (Human Meta-Analysis)
Verification: A systematic review and meta-analysis confirmed that low preoperative total testosterone is an independent predictor for Gleason score upgrading (finding more aggressive cancer than expected) after radical prostatectomy.
Source: Piao, S., et al. “Low serum total testosterone level as a predictor of upgrading in low-risk prostate cancer patients after radical prostatectomy: A systematic review and meta-analysis.” BMC Cancer, 2022.
Verification: This meta-analysis of 15 studies confirmed that while TRT does not increase cancer risk, it does cause a statistically significant increase in PSA levels (0.271 ng/mL for IM injections), which often triggers biopsies that might otherwise not have happened.
Source: Cui, Y., et al. “The effect of testosterone replacement therapy on prostate-specific antigen (PSA) levels in men being treated for hypogonadism: a systematic review and meta-analysis.” Medicine, 2015.
5. Claim: Supraphysiological doses of testosterone (Bipolar Androgen Therapy) are used to treat Castration-Resistant Prostate Cancer (CRPC).
Evidence Level:Level B (Human Clinical Trial / Phase II)
Verification: Trials demonstrate that rapid cycling between supraphysiological (high) and castrate (low) levels of testosterone can induce DNA damage in cancer cells and restore sensitivity to anti-androgens.
Source: Teply, B. A., … & Denmeade, S. R. “Bipolar androgen therapy in men with metastatic castration-resistant prostate cancer after progression on enzalutamide: an open-label, phase 2, multicohort study.” The Lancet Oncology, 2018.
Current data supports the counter-intuitive finding that prostate cancer cells are vulnerable to extremes: they thrive in a “normal” androgen environment but can be suppressed by castration (zero T) or supraphysiological shock (high T). The danger zone appears to be chronic low-normal levels, which may select for aggressive cell lines, rather than the high peaks seen in injection protocols.
My urologist and GP physicians think all is fantastic… and not likely to get prostate cancer due to my small, tight prostate… size… and low PSA… under 1.
I’ve talked to urologists that say the same thing. Of course, we can’t know for sure in every situation and all the Urologists said to check PSA annually when on TRT.
My n=1 (not myself) is the story of this arrogant colleague who had several ex wives who got into the hormone pushing racket. He died at 68 of metastatic prostate CA.
His urologist (forget HIPAA) told me he wasn’t checking his PSA and was like 300 on presentation. He died fairly quickly after the back pain started.
You can’t get around that the prostate is a cancer waiting to happen and that testosterone is the growth stimulant. But just like breast cancer in women, HRT is not as big an issue as feared. Perhaps saturation effect but wouldn’t want to bet my life on that effect being infinite - ie if you go really high, there is probably some increased risk.
Also heard that low PSA levels are very reassuring including trends - like if you were 2 at a young age and stay 2 - that is very reassuring. I’m in the stable .7 to .9 range so feel like T is a relatively safe option. If I was 4 and getting MRIs and biopsies, I wouldn’t chance it - or would have a much lower target range.
Thats exactly my point DavidC that you can never be certain. Like the saying goes, most men will die with cancer but not OF it. I have bloodwork and appts coming up shortly. Testosterone is a growth stimulant for prostate cancer IF you already have some. The older one gets the more likely it is. I am 75 so I got to be more careful than you younger guys.
My PSA has always been < 1.5 my whole life up until a year ago, but it has varied from .6 to 1.5 regardless of TRT usage. A year ago it went up to 2.5 when I started on Metformin so that may be a clue. A Uro told me that Finasteride lowers the PSA reading.
When I heard about the protective effect of Rapamycin and Autophagy as well as Longevity claims I thought that would be a good way to go. I just started Rapa this month. Does Rapa effect PSA?
Hey Dave… on both high normal weekly 200 mg TRT score 1400 and a daily 25 mg Jardiance SGLT2 Inhibitor. And, HGH 3.5 iu daily for 1 year.
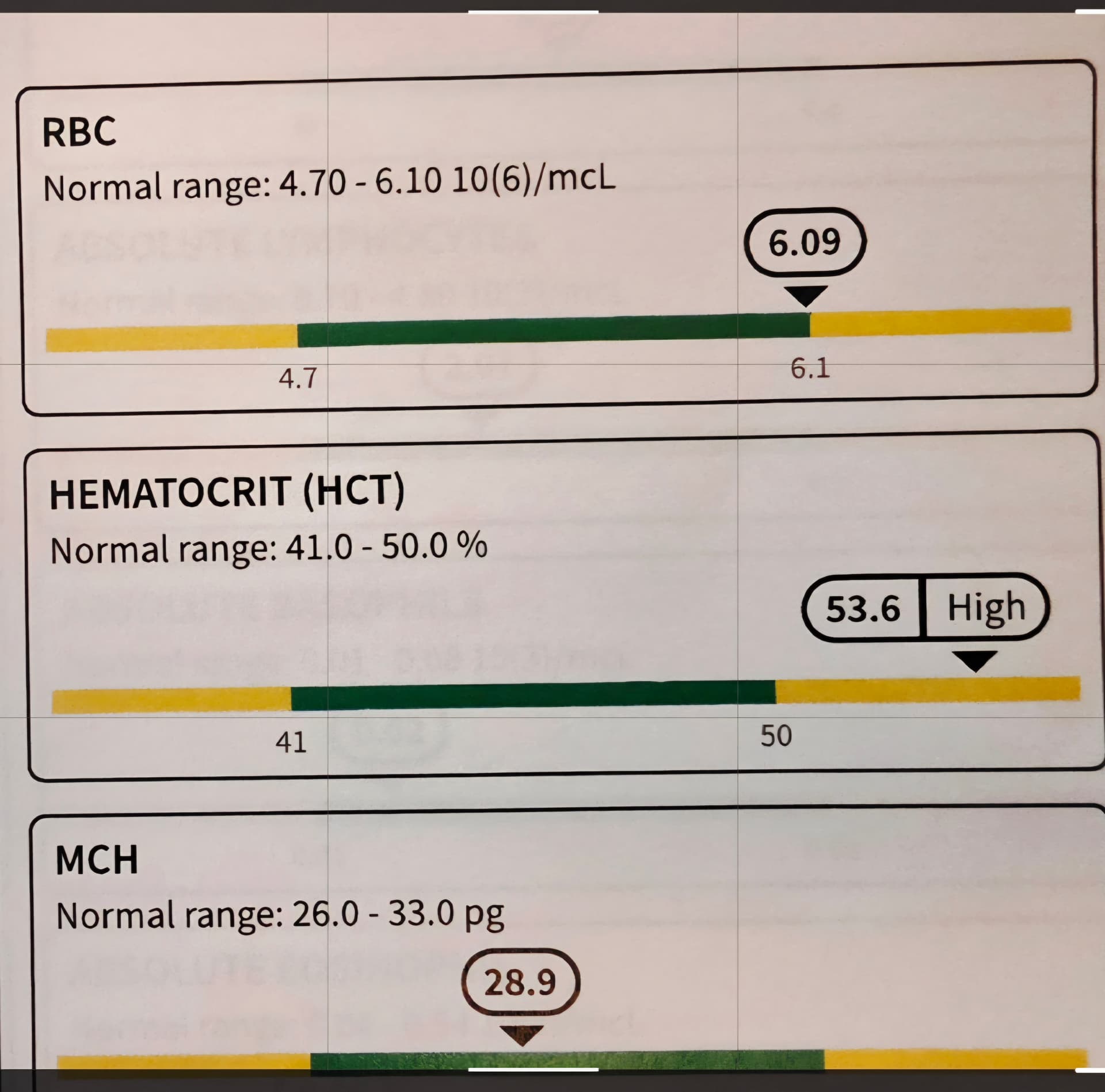
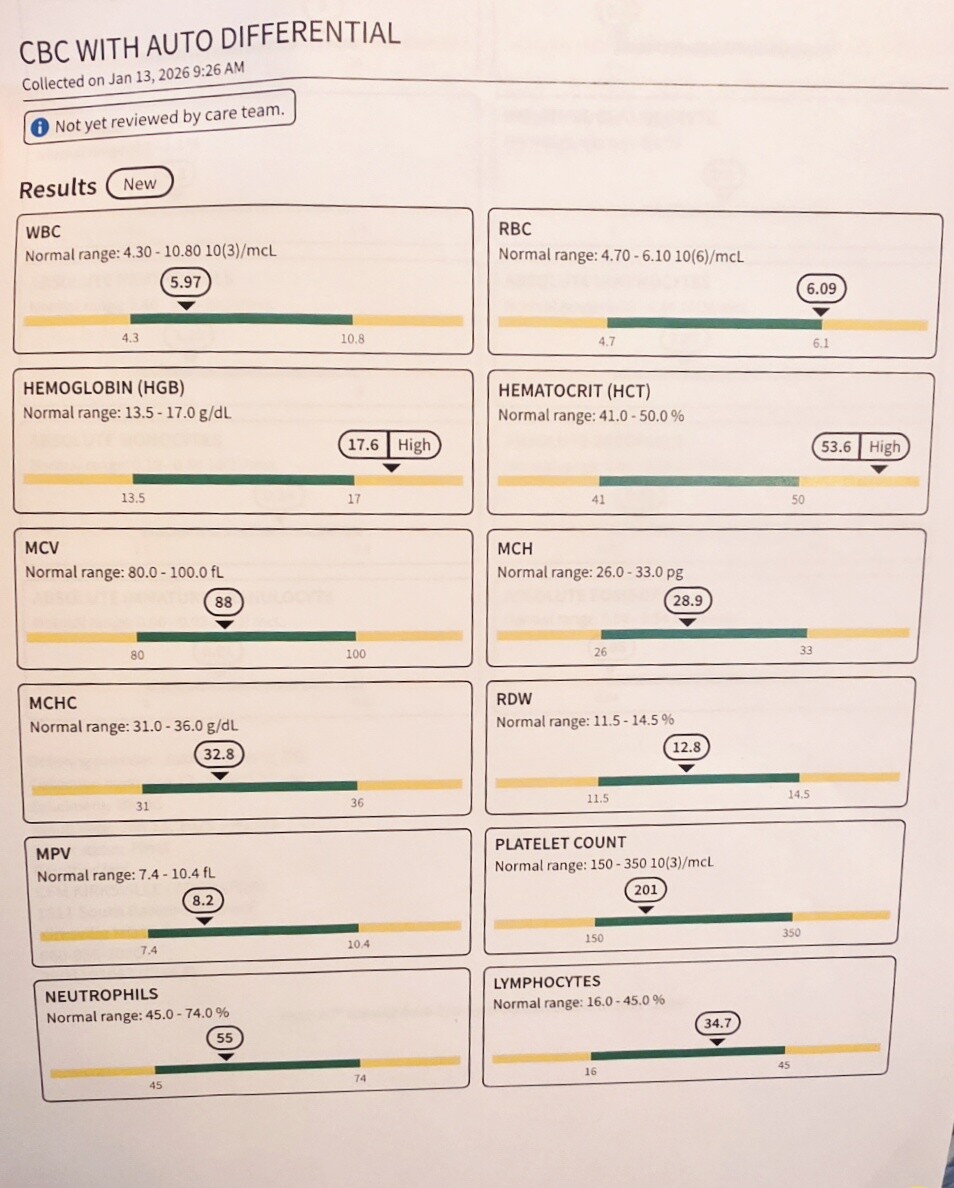
Even with all those – my hematocrit is in the almost normal range for adult males 42% - 52 % - I am at 53.6 my doctor says is fine for me, my muscles, weight and overall great health.
I think your doc is being a bit cavalier , maybe even reckless saying that 53.6 hematocrit is ok when the evidence clearly says the opposite. At least it sounds like, from your previous posts, that your other cardiovascular risk factors are low, so hopefully they offset the elevated hematocrit. I’m more conservative due to my calcium score, high Lp(a) and fam history.
I can see your point, unlike most on here, I have a 20 year friendship and a 6 year patient relationship… with blood panels and physicals every 3-4 months due to the longevity and healthy benefits I seek.
Long thoughtful approaches. Using current research… and a lot has changed in the past 6 years. More, openness… grey areas… as opposed to black and white… never attitudes… some things turning 180 degrees opposite.
Being seen as a unique person… and planning… monitoring regularly. With years of TRT… slight elevated hematocrit expected… we will discuss options.
True, having a Coronary Calcium Scan score of zero… 2 tests past 5 years… test 3 in a few weeks. Let’s see were it lands.