The evidence grows… and is getting harder! Lol
Cialis or generic tadalafil has great benefits to mens health in 5 area’s.
Here a quick overview, with excellent concise explanation. Going on 3 years plus… 5 mg daily rocks.
Link:

The evidence grows… and is getting harder! Lol
Cialis or generic tadalafil has great benefits to mens health in 5 area’s.
Here a quick overview, with excellent concise explanation. Going on 3 years plus… 5 mg daily rocks.
Link:
For pill splitting, I use a pill splitter like the one below.
A while back I used cypionate with Palmer’s Cocoa lotion for my face… until I ran out… it worked great. I have decided to give it another try.
what effects did you notice and how did you came to this idea? Never thought about using testo cream on my face ![]()
Hello Ludovic – I saw it here: https://youtu.be/hIY-G3sHbQA Check at the 9 minute mark in the video for cypionate 9:0
We know it is It is possible to convert testosterone enanthate, which is typically administered via injection, into a cream or gel formulation. However, this process should only be conducted by qualified professionals in a controlled laboratory setting, as it involves chemical formulation and requires knowledge of pharmaceutical compounding. I use a very fast absorbing lotion (Palmers Cocoa).
Key Considerations:
I like Palmer’s lotion because it is one of the oldest products with natural cocoa butter.
5 Reasons to fall in love with Palmer’s
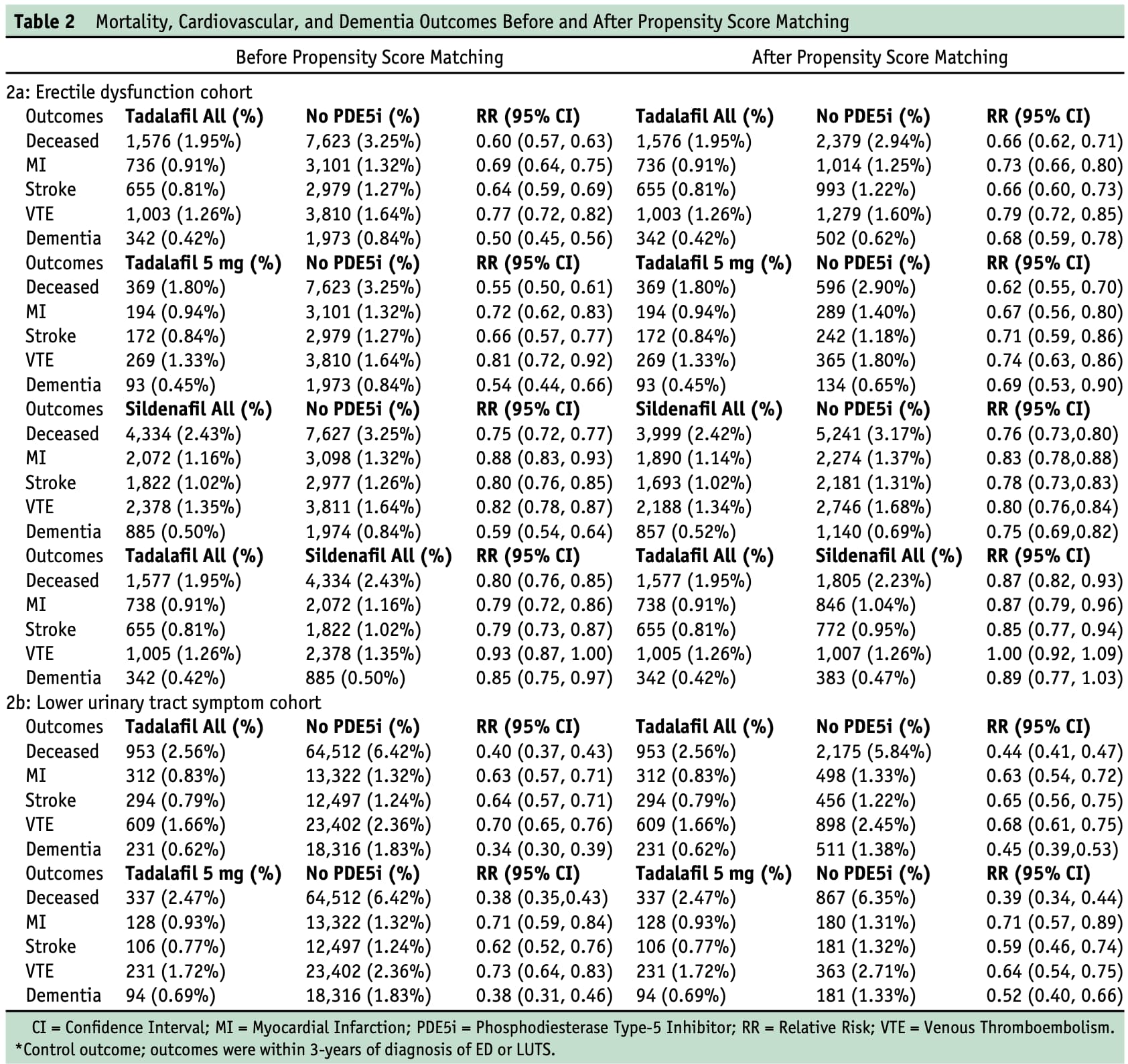
New paper from the future (march 2025!):
Benefits of Tadalafil and Sildenafil on Mortality, Cardiovascular Disease, and Dementia
The adjusted odd ratio for dementia is 0.68 (0.59, 0.78) in the ED cohort and a very impressive 0.45 (0.39,0.53) for the lower urinary tract symptom cohort.
Maybe the second cohort is more representative of the people taking tadalafil for longevity rather than ED.
Conclusion
Males 40 years of age and older with erectile dysfunction taking tadalafil experienced significant reductions in all-cause mortality, myocardial infarction, stroke, venous thromboembolism, and dementia compared to those not on the medication. Both tadalafil and sildenafil provided benefits, with tadalafil showing more favorable outcomes.
How Propensity Matching Was Applied in the Study
The study used PSM to ensure that the groups being compared (e.g., men on tadalafil vs. no PDE-5 inhibitors) were as similar as possible in terms of demographics and health conditions that could influence the outcomes. Here’s how it was implemented, based on the “Statistical Analysis” section:
Demographics: Age, race, ethnicity (e.g., White, Black or African American, Hispanic or Latino, etc.).
Pre-existing Conditions: Eight specific conditions were included:
Diabetes mellitus (ICD-10: E08-E13)
Acute kidney failure and chronic kidney disease (ICD-10: N17-N19)
Overweight and obesity (ICD-10: E66)
Cardiac arrest (ICD-10: I46)
Ischemic heart diseases (ICD-10: I20-I25)
Malignant neoplasm of bronchus and lung (ICD-10: C34)
Chronic obstructive pulmonary disease (COPD) (ICD-10: J44)
Hypertension (ICD-10: I10-I16)
These covariates were chosen because they are potential confounders—factors that could independently affect the likelihood of receiving PDE-5 inhibitors and the outcomes (e.g., mortality, cardiovascular events).
The propensity score was calculated using linear regression for continuous variables (e.g., age) and logistic regression for binary outcomes (e.g., presence or absence of a condition).
For each individual, this score represents their probability of being prescribed a PDE-5 inhibitor based on the listed covariates.
A 1:1 greedy nearest-neighbor matching approach was used. This means:
Each treated individual (e.g., a man on tadalafil) was paired with one control individual (e.g., a man not on PDE-5 inhibitors) whose propensity score was the closest match.
“Greedy” refers to the algorithm selecting the best match available at each step without reconsidering previous matches to optimize the overall balance.
After matching, the study checked the balance between groups by calculating the standardized mean difference (SMD) for each covariate.
An SMD less than 0.1 indicates a well-balanced match, meaning the groups are sufficiently similar. The paper confirms that “all of the standard mean differences of the covariates were less than 0.1” post-matching.
Outcomes (e.g., all-cause mortality, myocardial infarction, stroke, venous thromboembolism, dementia) were compared between the matched groups using univariate analysis (chi-square tests for categorical variables and t-tests for continuous variables).
Results were reported as risk ratios (RRs) with 95% confidence intervals (CIs) and p-values.
Limitations of PSM in This Context
However their quote sounds like socioeconomic is only 1-4% effect, which seems very low to me?
“Socioeconomic factors, such as Medicaid coverage limitations on lifestyle drugs, could influence medication affordability. Our posthoc analysis suggests these factors have minimal impact with only a 1%-4% difference in relative risks.”
I think it’s a wonderful drug. I can’t say for sure, but I believe it gives better pumps in the gym. I also heard the urologist on the Attia podcast explaining that Tadalafil is almost “exercising” the penis by keeping the vessels responsive.
I believe Viagra is currently being tested by the ITP right now, so we’ll see whether effects on blood pressure, large vessel NO etc translate to longevity. However, even if there’s no positive effect on lifespan, IMO this is a drug with big quality of life (thus healthspan) benefits.
Just psychologically, being able to have a “full” erection every time is fantastic, even just from an ego-driven point of view. I never had any real problems before, but with Cialis (or Viagra) you can achieve a level of consistent hardness which is very satisfying, both for yourself and your partner. I also wake up with erections much more often when using it.
I understand that they looked at people who were prescribed tadalafil or sildenafil once in a 6 month period post diagnosis (of ED or LUTS) and then magically these people get better compared to those who did not? It sounds weird to me. We don’t even know if these people continued to use the drugs. We also need: the survival curves (other PDE5i papers with these curves were not convincing) and the dose response relationship (if taking sildenafil once at low dose is as good as many times at high dose, then there might be confounders…)
It looks like they didn’t control for other drugs. Which is bad when we know all the research showing that alpha blockers might be neuroprotective.
Even more so considering that Mendelian randomization shows an INCREASED risk of dementia with PDE5i: Large Study Finds Viagra Is Linked to Almost 70% Lower Risk of Alzheimer's - #129 by adssx
I want to believe but I’m very skeptical given the confounders + the MR study + the poor quality of the research.
It’s an epidemiological study with all the usual caveats but:
On the other hand concerning the MR study:
Anyway, even if the genetic proxy for PDE5 inhibition were a valid one, the observed benefit could be due to something entirely different. For instance, just as a totally hypothetical example, it could be that the ED cohort taking tadalafil have a better sex life so they are happier and that it’s that happiness that has positive benefits and not the PDE5 inhibition. Or it could be that the inhibition is pulsatile, or tissue specific, etc.
Does a larger cohort reduce residual confounding?
If you just hear the dataset: people 57 years old over a 3 year period who have taken tadalafil have a decrease in mortality, that already is low, over the 3 year period, okay.
It’s not convincing to me at all, the only way it is if listing the odds ratio makes me think it’s an RCT or MR.
Lots of conflicting data when it comes to dementia, so not, it’s not like all studies are going in the same direction: Large Study Finds Viagra Is Linked to Almost 70% Lower Risk of Alzheimer's - #129 by adssx
As far as I know, in guidelines, tadalafil is prescribed in LUTS if people also have ED. It’s not a first-line drug for LUTS. So, who are the people in this dataset with LUTS but without ED who are prescribed tadalafil? Did they try other drugs (such as alpha-blockers) and it failed in them or they didn’t like the side effects and then they switched to tadalafil? Or is it that in reality they have ED but they were shy to disclose it or they didn’t want it to be written in their medical records or their doctor didn’t want them to feel ashamed by it? Or is it that they complained about mild LUTS to their doctor and the doctor asked “Do you have an active sex life? How is it going?” and they answered that they wouldn’t mind a little boost?
It’s not like comparing ACEi to ARBs. Someone who is given tadalafil for LUTS is most likely very different from someone who is not: probably a milder course of the disease + in a relationship + with an active sex life + pro-active when it comes to talking to a medical professional about their medical problems.
That’s why I find these association studies around PDE5i hard to analyze. And even more so when they don’t adjust for other medications + other conditions (especially mental health ones) + don’t look at the dose–response + don’t show the survival curves. Survival curves might be the most important: For me, if a drug is protective, we should see that the longer you take it, the better, and the curves should separate more and more over time, often you see the separation after a few months and it stays constant: that’s a red flag indicating confounders (I might be wrong, my two cents…).
When you combine this to the MR (yes a preprint, but Oxford) that’s not great.
That being said, I’m mostly talking about neuroprotection. For cardiovascular health, there was one good paper about tadalafil with great dose response charts.
I agree, we all focus on what is most important for us. ![]() I do have severe CVD so I’m more focused on the cardiovascular aspects.
I do have severe CVD so I’m more focused on the cardiovascular aspects.
Actually I was wrong, in the European guidelines on LUTS, PDE5i are also recommended to men without ED (“Use phosphodiesterase type 5 inhibitors in men with moderate-to-severe LUTS with or without erectile dysfunction: Strong”): EAU Guidelines on the Management of Non-neurogenic Male LUTS - Uroweb
But it would be good to look at the “non-PDE5i” group: are they taking tamsulosin (not great), other alpha-blockers (potentially great), 5-ARIs, beta-3 agonists, or muscarinic receptor antagonists?
The advantage of PDE5i might come from one terrible drug in the “non-PDE5i” group.
I am 44. I am plant based with strong erection.
I want to use it as a gym pump, but I’m afraid of Priapism.
Exactly. This isn’t a free lunch for those who use it who don’t have ED, intuitively risk might be higher to use it without ED.
Grok 3 disagrees with you
" General Population
In the general population, priapism is very rare. According to studies, the incidence (number of new cases per year) is about 1.5 cases per 100,000 people annually. This means the rate is less than 0.0015% per year in the general population. However, many cases might go unreported because people don’t seek help due to embarrassment or spontaneous resolution.
Among Viagra Users (PDE5 Inhibitors)
For men taking Viagra or similar drugs (PDE5 inhibitors) for erectile dysfunction, the risk of priapism is slightly higher but still very low. Based on clinical trials and side effect data:
In controlled studies with over 14,000 men taking Viagra, priapism was reported in 0.1% of cases (1 in 1,000 people).
In post-marketing data (after the drug’s release) with over 39,000 men, the rate was slightly higher but still below 1%.
Specific High-Risk Groups
For people with certain conditions, like sickle cell anemia, the risk is significantly higher:
Conclusion
In percentages, for the average Viagra user, the chance of priapism is below 1% (more precisely around 0.1% according to clinical data). In the general population, it’s even lower, below 0.0015% annually."
I mean to use it without having erectile dysfunction. If you have normal erections and add tadalafil on top of that, compared with having ED and add it on top, which has higher risk of priapism? And by how much?
Priapism simply isn’t happening with PDE5’s, especially not at the low daily doses being discussed. We aren’t talking about trimix injections here. 0.0015% like Chat gpt says above sounds about right, and I’d assume that’s with huge doses. It’s just not something to worry about.
Those stats are those with ED. What’s the number for off label use?