That said that’s a huge risk increase for the US calculator.
Note that if I plug the values with the lower LDL in the US calculator, I get 6.7% which is basically almost identical.
I think you raise an interesting point. And I’m fascinated what people think of these statements all of which I happen to believe (but with varying degrees of confidence!). I think it might help tease out our biases.
Apo b is a necessary factor in atherosclerosis
Higher Blood pressure mechanistically increases the risk of apo b damaging blood vessel walls
Statins have clear side effects for some people.
Statins may have unclear side effects for others and so minimizing the necessary dose is sensible
Statins have a clear net benefit in secondary prevention
Statins have a population level net benefit in healthy 40+ year olds if taken for long enough
Most of the apo b impact of statins can be replicated by lifestyle and nutrition
We don’t know for sure what apo b to target, but it’s a lot lower than typical western diet population level, and is likely to be sub 70 mg/dl
Apo b is not a sufficient cause of atherosclerosis
Low inflammation or other factors may be protective against atherosclerosis in the presence of high apo b.
Though your LDL values are now higher (198 vs 106) your HDL values are also higher (95 vs 59) and higher HDL values can lower CVD risk more than a similar decrease in LDL. This is even more true for the ApoB and ApoA values. High ApoA (approximated by HDL) values, even seem to be able to reverse Atherosclerosis.
Any idea what you did to raise your HDL that high ?
The change in cholesterol happened when I switched my diet to low carbs and started endurance training (running) at the same time 3 years ago. At the beginning, I went full Keto (basically no carbs) while running fasted in the morning to switch my metabolism to burning fats instead of carbs.
I have the Lean Mass Hyper Responder (MLHR) phenotype. That phenotype is defined by LDL 200+, HDL 80+ and TG < 70. Also my VHDL is too low to be measurable. The theory is that you need more cholesterol particles to transport the fats as a fuel but they are not atherogenic.
There is an ongoing study to see what the effect of those lipids is on plaque formation. The preliminary results are very good. LMHR people with an average LDL of 270 (but very high HDL and low TG) have less plaque than matched controls with low LDL. The subject with the highest LDL (500+) has no plaque at all.
The basic model is that inflammation (or injury) to blood vessels causes LDL to deposit plaque (as a kind of bandaid), but normally once the inflammation/injury resolves HDL dissolves the plaque and carries away the cholesterol from the plaque. In CVD, for some reason, the plaque becomes permanent and keeps growing.
I disagree. I enjoy reading smart posts and drawing my own conclusions on both sides. I used to live in a bubble and believe the “statins are poison and will kill you” crowd until I heard the other side which was much more evidence based. I wish I had been taking a statin from a young age instead of listened to them.
It seems clear statins have benefit but it’s over the long term, hence why this meta analysis doesn’t show a significant reduction in mortality risk. Atherosclerosis takes much longer than 3.7 years to manifest.
It just makes too much sense to start a low dose Rosuvastatin at a young age and then probably not have to worry about atherosclerosis much later in life.
Seems the negative studies have patients starting them way too late. Kind of silly to wait until you have a high calcium score to use one. Prevention is key.
Some excerpts in addition to @tananth 's summary:
Once LDL (APOB particles) enters a wall lesion, it has to be oxidized then that starts an inflammatory cascade. HDL is part of several mechanisms trying to fix that.
Surprisingly, native LDL […] has to be modified to promote foam cell formation. Oxidative modification converts LDL into atherogenic particles that initiate inflammatory responses. Uptake and accumulation of oxidatively modified LDL (oxLDL) by macrophages initiates a wide range of bioactivities that may drive development of atherosclerotic lesions.
The precise mechanisms that generate oxidized lipoproteins in vivo are still only partially understood. LDL circulating in the plasma appears to be protected from oxidation, both by dietary antioxidants such as vitamin E and C (259) and by protective enzymes including glutathione peroxidases […]
In contrast, an atheroprotective function of HDL is to prevent endothelial activation and enhance NO production to maintain barrier integrity
In addition, HDL maintains plaque stability by inhibiting degradation of the fibrous cap extracellular matrix through its anti-elastase activity
HDL, apoA-I, and endogenous apoE reduce lesion formation by preventing endothelial cell activation, inflammation, and oxidative stress and also by promoting cholesterol efflux from foam cells.
Again my point is not that statins are intrinsically bad but they are just one tool and that this is much more complex than the simplistic view of high LDL is bad and everybody should take them.
Not to forget that all the cause mortality as well as the centenarian studies show that a very low LDL is not optimal.
However, if you have high levels of LDL floating through your system and you happen upon an inflammatory event (which is hard to avoid 100% of the time) you may develop the plaque as your body treats the inflammation with calcification. Not an ideal situation, and very hard to avoid without maintaining low levels of inflammation (almost impossible) or LDL and ApoB (much easier with medication).
So, it’s much easier to go with treating LDL and ApoB than to make sure you never have an inflammatory event.
While statin treatment to lower LDL seems to be the drug class with the greatest effect on lowering CVD, the anti-inflammatory Colchicine (discussed in other threads) reduces CVD by 31% (in those without CVD history), which beats all LDL lowering methods (other than statins), including PCSK9
Very interesting. What’s your personal supplement/pharma strategy? Do you try to focus on both ldl/apo b and inflammation? Or just inflammation and boosting hdl?
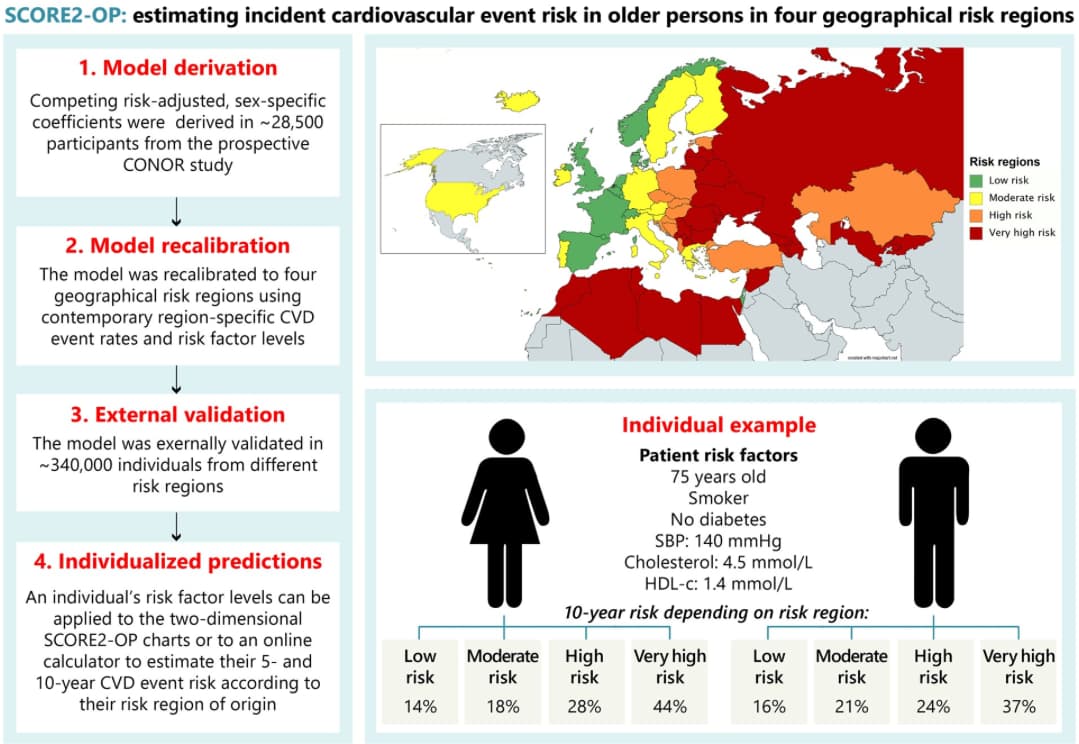
On the CAD calculators and risk score … really an irrelevant item as for each of us, our N=1 is what matters. The current approach is illogical. So you can see your doctor on Monday and be told no need for lipid treatment with your age of 55, a bit of hypertension, overweight, sedentary with an LDL of 150, and an APO B of 125. On Tuesday you have a stroke or heart attack - now suddenly, 1 day later your LDL (which we shouldn’t even be using) goal is <70 mg/dL. Why a day earlier was 150 okay, now <70 is required? Furthermore, lets say you have an Lp(a) if you doctor even knows to test this … now your goal if for an APOB<50. Same person … only difference is your doctor watched you develop vascular disease, and now that you have an adverse outcome and have it all through your vessels …the goals change.
My point on the calculators is that I don’t use them at all - I look at individuals and optimize their personal risk. So the discussion on the calculators above is interesting, but on a personal basis, they are irrelevant - if you aren’t optimizing your risk you are daily increasing damage to your vessels and at some point will potentially have an event that could irreversibly impact your life. Avoiding this before it happens is important.
Doesn’t matter how you get a low APOB … diet, exercise, drugs of any type that you tolerate, but optimizing this, blood pressure, glycemic control all pretty important. I’m happy that folks have brought up a lot of different strategies for this, and statins aren’t the only strategy, they are just the most common and cost effective.
If people are so terrified of statins (as a result of listening to bad advice), they could at least take Ezetimibe to lower ApoB. I took ezetimibe first before adding 5mg Rosuvastatin and let me tell you, Ezetimibe has a strong effect at lowering ApoB by itself.
Some people are afraid of statins due to fearmongering, others outright deny the role of cholesterol in heart disease due to conspiracy beliefs and/or being keto/carnivore enthusiasts who believe that because they are “feeling good” and are losing water weight, their diet must be the best one there is and also cures every disease in existence. So when cholesterol goes up due to high saturared fat intake, that can’t be a bad thing therefore science must be wrong.
This is not necessarily true. Overweight and obese people, especially those who do not exercise are likely to have high cholesterol because of their high intake of fats and sugars.
Many people on the Atkins and Keto diets do not have high cholesterol. I think people who exercise and maintain a good BMI will probably see no effect on cholesterol from a relatively high saturated fat intake such as found in meat and dairy products.
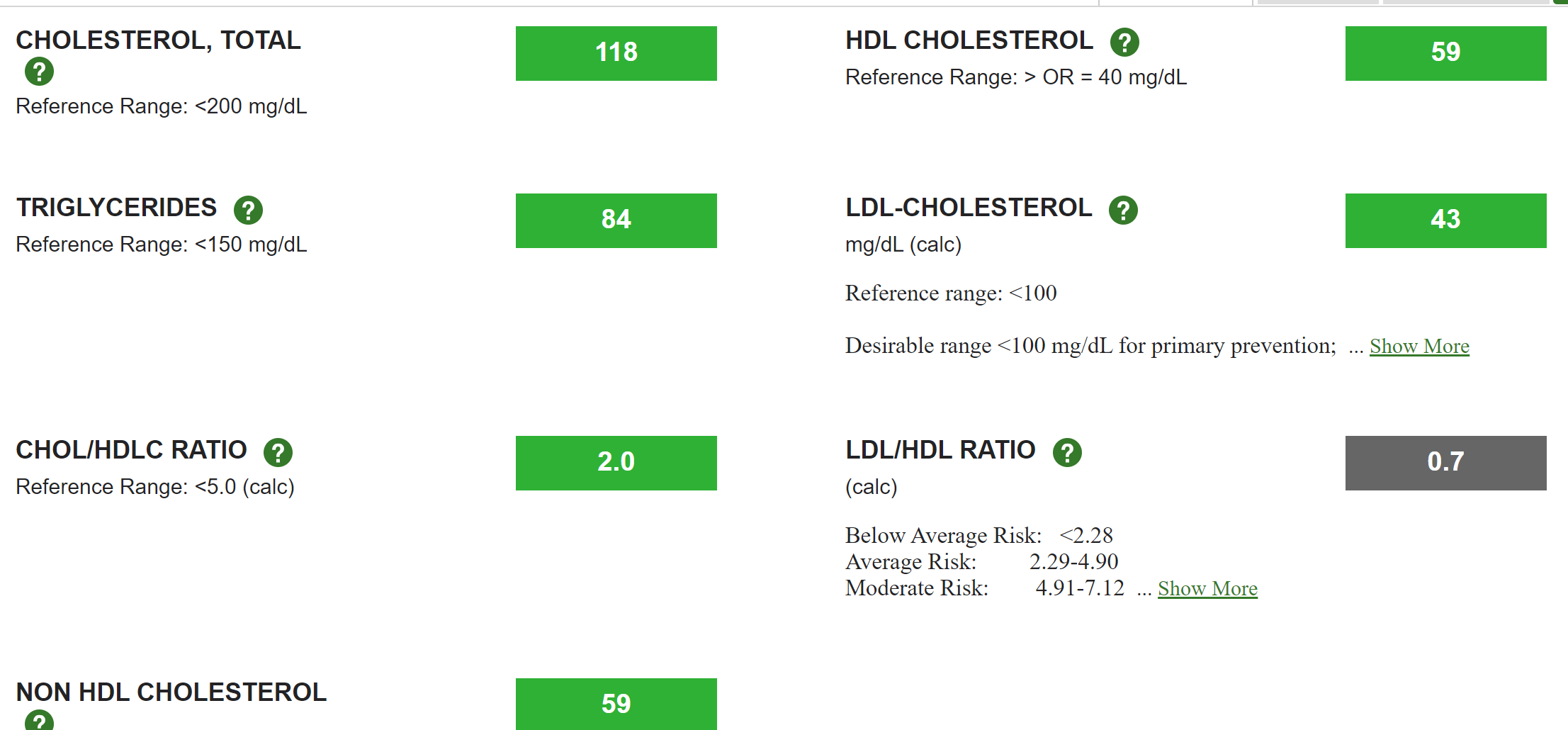
Personally, I have a fairly high intake in the form of meat and dairy products, and my LDL, triglycerides, and HDL are close to optimal.
I do take a statin and ezetimibe and Pantethine.
From a vascular standpoint, so long as you have had these numbers for some time, and you have reasonable glycemic control and goal your blood pressure in the 115-120/70-75 mmHg range … I don’t think a stroke or heart attack with be your cause of death or disability!
Having a diet high in meat and dairy however elevates a common cause of death - malignancy.
Amazing lipids however, and if you’ve not had numbers like this for a long time - once you hit 5 years of this, it would seem like the number 1 & 3 cause of death and disability (heart attack and stroke respectively) will not be a worry. So good for you that you’ve mastered your lipids!
I’d love to know your APO B - which really is the only item you should measure - I’d suspect it’d be in the 50’s, which is great!
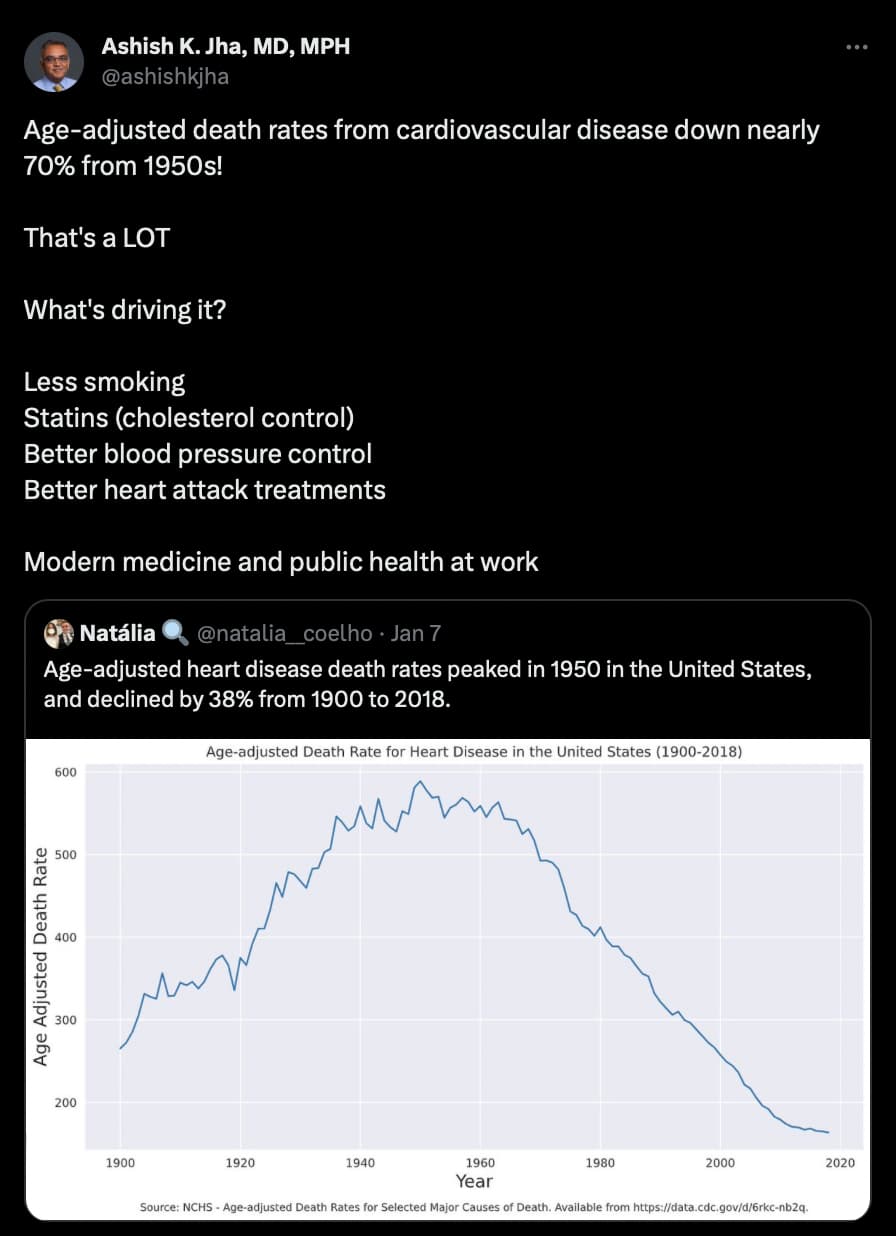
Ford et al. (2007), looking at data from 1980-2000, estimated that “47% of this decrease was attributed to treatments,” and 44% to “changes in risk factors, including reductions in total cholesterol (24%), systolic blood pressure (20%), [and] smoking prevalence (12%)”