I have a great experience with Anil from Kachhela, he notified me the minute he got the payment using wise, and he sent me a tracking number for the the shipment.
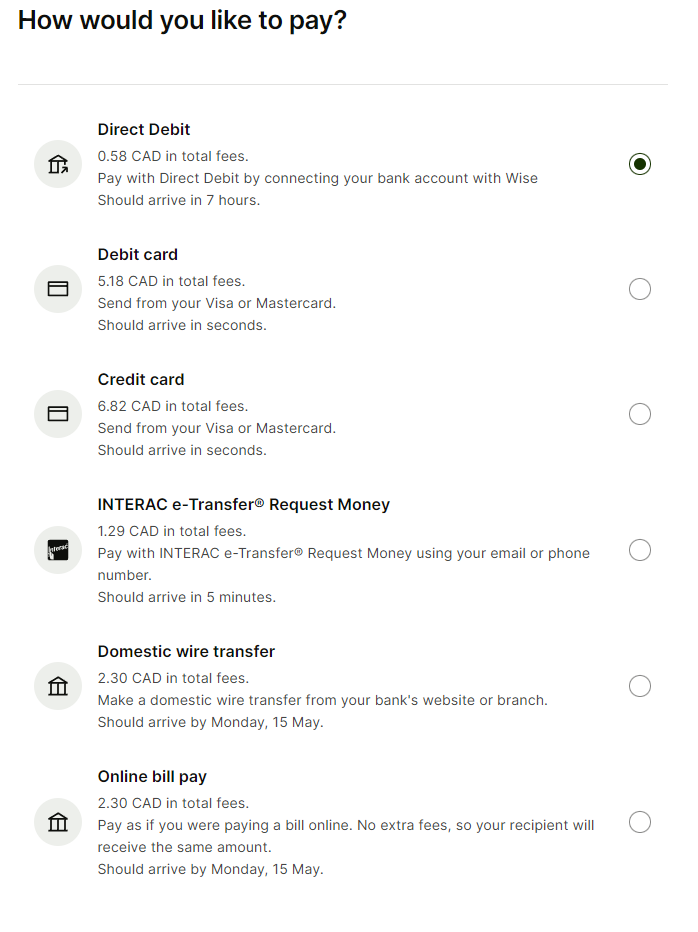
Using Wise is easy and can save you some time and money, you have to understand that first you need to fund your account and then you need to add a recipient:
I used interac etransfer from my bank and it was really fast (about 20 minutes for the money to arrive)
I already referred 2 friends to Kachhela, we live in Canada and had no issues at all. We all ordered 300 pills of Siroboom.
Before sending the money, I notified Anil by email that I was going to proceed with the payment and send him my full name and address.
If by any chance you haven’t opened your Wise account yet please use this link to get a discount:
Let me know if you have any other questions and good luck!
Wow! That’s a huge difference. Can you share how close to exactly 2 hours you were on all 4 tests? Also, aside from the one time with gfj were these all totally empty stomach first thing in the morning or was there food or evoo involved?
I have always taken my rapa at 9:00 a.m. for an 11:00 a.m. Labcorp appointment. The appointments have never been late- all of the tests were within a minute or two of two hours.
All of the doses were taken on an empty stomach- although I swallowed 1+oz EVOO with the 8mg dose that registered 12.9 (EVOO slows absorption? I read that someplace on this site)
I guess I’m hoping this is just an anomaly- I have 100 of the 2mg Siroboon pills and I’m pretty sure I can’t return them to IndiaMart!!! I’m thinking I might need GFJ to get them up to the desired range.
Sounds like you’ve tested very close to 2hrs with all of your labs. I don’t see how a level of 3.1 can be possible other than the siroboon being much weaker than the rapacon. I wonder has anyone else on this forum taking siroboon has tested a peak?
We were just discussing why people shouldn’t be having their blood drawn two hours post dosing in another thread.
Also, the study mentioned in post 2 of this thread used Sirolimus liquid solution rather than enteric coated pills.
Pfizer has stated it takes an average of three hours to reach Tmax after healthy persons take the tablet on an empty stomach. “Following administration of the sirolimus tablet, sirolimus tmax was approximately 3 hours after single doses in healthy volunteers.”
But this is for Pfizer’s tablets. There’s no guarantee that tablets from other manufacturers dissolve and get absorbed at the same rate.
My suggestion is that people wait five hours before having their blood drawn. Or longer.
I am personally on board with the idea that trying to directly target t-max is just too difficult. It’s better to have the sirolimus level drawn at 48 hours and then extrapolate the t-max from the data we have available to us (as described in the link above). And, it would be great if hitch would do that. But, just based on the info he provided there are very few possibilities. It could have been a lab error (unlikely). Or, it could mean the siroboon didn’t peak yet (seems strange it the level didn’t get a little higher than it did after 2hrs). Or, it’s weak.
Well, as I just noted, Pfizer said the Tmax for their tablets on an empty stomach averages three hours. Plus, Pfizer uses nanocrystal technology, and part of the advertised benefit is “quicker onset of action.” That’s why I suggested waiting a minimum of five hours for other brands. Or even the following day for comparison purposes.
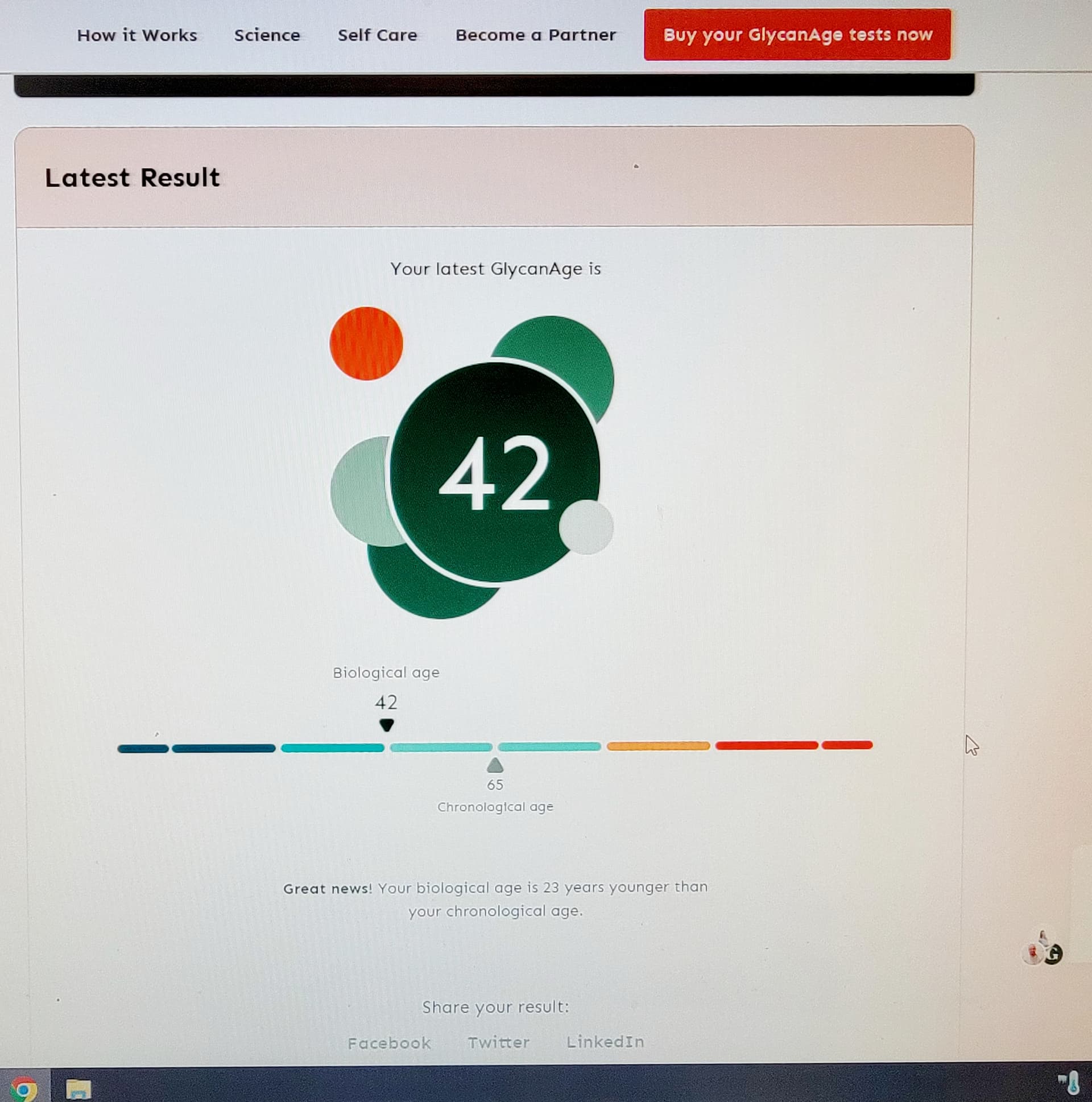
In case you didn’t see this post… after going on 36ng/mL for 7 months… based on Mikhail Blagosklonny recommendation to go high as possible with no side effects. You can have silent pathology. My biological markers aged decades… not good!
From Matt Kaeberlein who is the best: “I absolutely think it’s possible that 36mg could be net detrimental to health while 6-8 mg could be beneficial. I am certain the optimal dose will be different for different people.”
I am fairly typical and those high doses were not good for me N=1. I reduced back to 6-8 mg and my biological markers went back to a younger age… took 8 months to get there again.
You are getting high doses in your blood based on you measurement… but does that equate to positive health benefits??
The argument of high doses to cross the blood brain barrier… Matt Kaeberlein shoots down too. Saying peripherally the reduction of brain inflammation may be enough.
“I am fairly typical and those high doses were not good for me N=1. I reduced back to 6-8 mg and my biological markers went back to a younger age… took 8 months to get there again.”
Which biological markers? Was Glycanage one of them?
Holy shit, I’ve also been using high rapamycin doses [there’s some evidence they’ve done more harm than good - my 2020 blood tests, before I used larger-than-small doses, were near-ideal on all dimensions], and will dial back (though I also have semaglutide now, which is probably better for me than rapamycin)
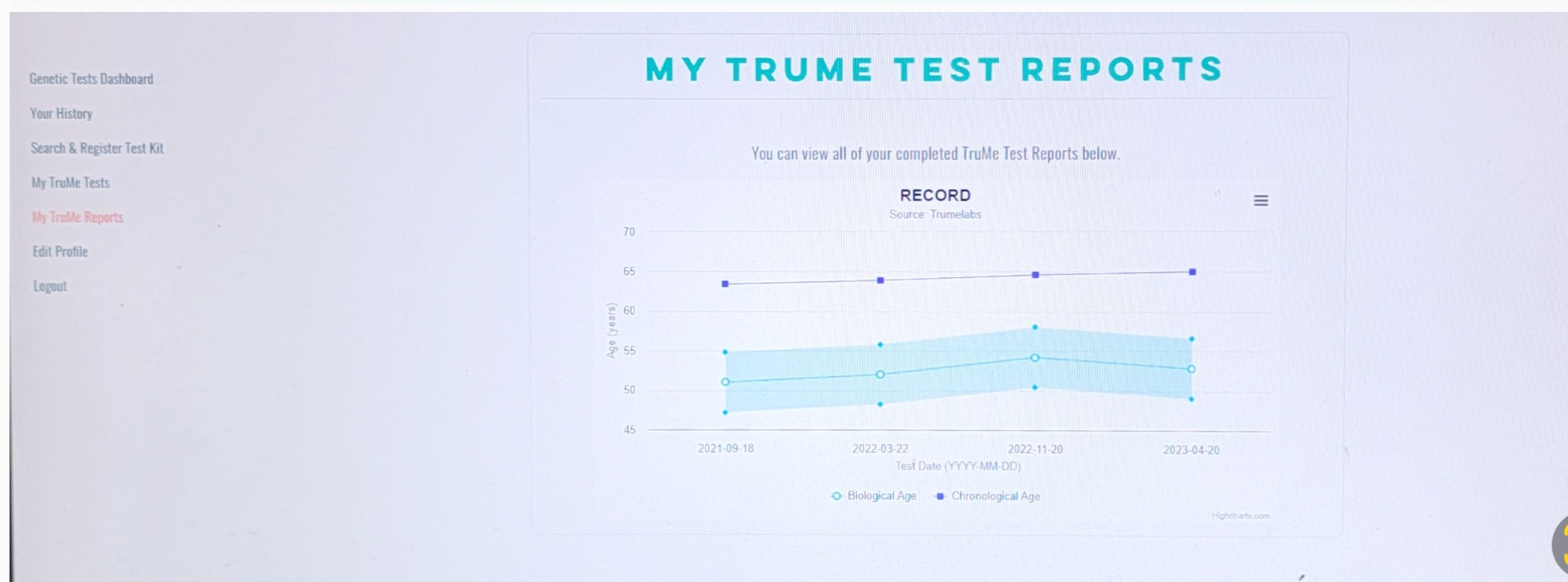
Is TruMe just the 1st-generation epigenetic aging clocks (Horvath/Hannum)?
As with all epigenetic tests, TruAge measures the amount of methylation of your DNA at certain regions that have shown a link to ageing. Their lab uses the bisulfite conversion techniquw; one of the three common methods along with differential enzymatic cleavage of DNA and affinity capture.
TruAge analyses the DNA methylation (DNAm) profiles of 9 small regions (loci) of DNA. For comparison, the original Horvath clock uses 353 CpG sites and his latest GrimAge clock uses 1,030.
So maybe 9 sites seems a bit low, however, even GrimAge only uses a fraction of the
28 million CpG sites in the human genome. There will always be a statistical error, and TruMe labs claim that their studies show an error margin of 4.6 years.
NOTE: the TruAge Explorer saliva test shouldn’t be confused with the more expensive ($399) TruAge blood test from TruDiagnostic which uses 900,000 methylation loci to determine your biological age.
I asked Matt Kaeberlein about increased biological aging correlation.
Matt said this: : Rapamycin dose - I honestly don’t know. I understand Misha’s (Blagosklonny) rationale for pushing it as high as possible until you get to side effects. My concern there is that you might be getting to side effects and not know it right away or at all (silent pathology) until it’s too late to reverse the damage. I have no evidence for that, but it’s a concern I have.
I absolutely think it’s possible that 36mg could be net detrimental to health while 6-8 mg could be beneficial. I am certain the optimal dose will be different for different people.
I find it a little hard to reconcile the data we have from animal testing, with the issue of potentially negative impacts at higher dosing of rapamycin. I’m not saying it may not be true, I just don’t understand how it would be happening, and at what seem to be comparatively low doses … e.g. 36mg/in one weekly dose. It needs to be explored/researched more, that is for sure.
It seems that the mouse studies would suggest that we have a lot of headroom to explore in terms of higher dosing regimens (aside from the immune suppression issue). Per the data below: