Sure:
It’s the paper that the thread was started with, see above
Sure:
It’s the paper that the thread was started with, see above
As a reminder, empagliflozin extends lifespan as well in mice (at a dose way too high, TBD if a lower dose would increase more): Empagliflozin rescues lifespan and liver senescence in naturally aged mice 2024 (“Further exploration discovered that empagliflozin increased the concentration of SCFAs, decreased the levels of the inflammatory factors TNF-α, IL-6, and CXCL9, and regulated the PI3K/AKT/P21 and AMPK/SIRT1/NF-κB pathways, which may represent the underlying mechanisms involved in these beneficial hepatic effects.”)
AMPK is also activated by dapagliflozin: Dapagliflozin restores autophagy and attenuates apoptosis via the AMPK/mTOR pathway in diabetic nephropathy rats and high glucose-induced HK-2 cells 2024
In C. elegans, no SGLT2 increased lifespan: Million Molecule Challenge Results and Leaderboard – Ora Biomedical, Inc. (But I think the dose was too high and I sponsored another experiment at 5 µM, my bet is on dapagliflozin)
So the case for canagliflozin over empagliflozin and dapagliflozin seems very weak to me. Even more so considering that dapagliflozin and empagliflozin have a better safety profile than canagliflozin and are linked to better outcomes in RCTs and association studies (including on dementia).
For cancer, this 2017 blog post (I have no idea how reliable it is) concludes:
Based on the above you could argue that we should chose between e.g. Dapagliflozin and Canagliflozin depending on the tumor size and glucose status in the body.
Therefore, Dapagliflozin may be more relevant for the very large tumors, while Canagliflozin may be more relevant for smaller tumors in people with high blood glucose levels (e.g. who do not follow a low-sugar diet and do not use other glucose lowering medication).
@adssx Have we seen any Mendelian Ranomization for SGLT2i yet?
That we have that for SGLT1i (together with multi ITP studies on Cana vs the single somewhat weird one-off study on Empa) does still hold some weight in the direction of Cana if one’s goal is lifespan extension and longevity, and not just health improvement.
You’re right; the SLGT1 MR study gives one point to canagliflozin.
For SGLT2, we have this one: Canagliflozin - Another Top Longevity Drug - #1067 by adssx “Our study supported that SGLT2 inhibition increases father’s attained age, cognitive function and intelligence, which was mediated through brain images of different brain regions.” (males only again!)
And for SGLT2 and CVD & MI, we have these:
RCT’s and MR is the only way.
(and maybe mice longevity studies)
How would you see if cycling on and off works via MR?
Seems like we perhaps can use MR + mechanistic understanding of MR points to general benefit (which it does for SGLT1)
How is SGLT1 different now that we have an MR for SGLT2 and male longevity as well? SGLT2 Inhibitor Canagliflozin eliminates senescent cells and alleviates pathological aging (in mice) - #13 by adssx
I’m not an expert, I only have surface level understanding of MR. I’m not personally interested in any mouse, human, yeast, or cell mechanistic papers with buzzwords like “senescence”, “inflammation”, “metabolic dysfunction”, “mitochondrial function”, “neurogenesis”, “BDNF”, and other ones.
Not sure that it is different. Did not say it is different in my post you are referring to. But I have not yet read the SGLT2i paper and the abstract of the paper felt weird/i’m not understanding it yet so don’t want to tell people in a post that we have (good) MR analysis of SGLT2i before I have studied it and know if I believe that we have or not.
SGLT2 inhibition was associated with longer father’s attained age (years of life increase per SD (6.75 mmol/mol) reduction in HbA1c levels = 6.21, 95%CI 1.95 to 11.15)
Is that relevant for people in a normal range - or it just saying that people with massively higher HbA1c live shorter than those with massively lower HbA1c?
As mentioned, I have not yet been able to read the paper, so I just don’t know what it means yet
Come on man - don’t spin things. You totally know how that MR is a lifelong average exposure type of thing and hence cannot distinguish between a constant vs cyclical dosing.
I’m not knowledgeable enough to conclude on this. They note at the end:
Fifth, using a genetic variant in SLC5A2 to proxy the pharmacological SGLT2 inhibition, a recent study reported the cardioprotective effects of SGLT2 inhibition ([62](javascript:;)). However, the effects may not be attributed to lower plasma glucose since only a minimal mediation proportion was found. As our instruments were selected based on the HbA1c-lowering effect of SGLT2 inhibition, we should view our results with caution.
But they also write:
SGLT2 inhibition was associated with changes in the right supraorbital sulcus area (beta = 1.84, 95% CI 0.40-3.28, P = .01) and thickness of the paracentral area in the left hemisphere (beta = 1.52, 95% CI 0.08-2.96, P = .04), both of which led to an increase in father’s attained age (beta = .014, 95% CI 0.001-0.028, P = .04; beta = .023, 95% CI 0.004-0.042, P = .02). (Fig. 3 and Supplementary Table S4) (36). An indirect effect via these 2 IDPs accounted for 9.8% and 12.8% of the total effect between SGLT2 inhibition and father’s attained age (Supplementary Table S5) (36).
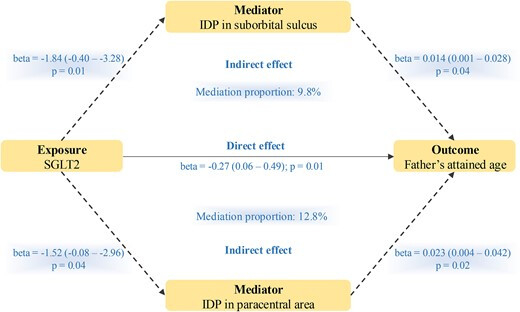
So I understand that ~80% of the increased lifespan (of the father!) is due to HbA1c lowering (“direct effect”) and 20% to indirect effects.
Is there a better way to do an MR study on lifespan?
I don’t know if I’m not an expert… I can think of situations where there can be cyclical effects from gene variants. There’s no spin, just a response to your question.
If you can’t find MR or RCT’s then maybe you don’t have enough evidence unless you think the expected benefit outweighs the risks. I’m not going to look or investigate all of those +EV bets if they are small as that’s too much cognitive load… Pascal’s Mugging Spam. And why I tune out from anyone or any studies using a bunch of buzzwords.
But the MR could not capture that at that level
Can turn it on so you can accept DM messages, tried to send you one but it did not go through because not accepted
Hello, I have been researching the various ‘reliable’ larger pharmacies in India shared on this site and sent several emails to a few of them requesting price and product quality verification. However, thw casual way they responded still makes me a little nervous about taking the plunge. Not concerned with not getting the product but even with branded products like empa worried it’s not the real branded product. Can you share whom you have had a positive first hand experience with please. Thanks!
I have had positive experiences with Jagdish Nikose and Maulik. Both have provided extremely good quality and value. I have used both several times.
Here are their WhatsApp contacts
Thanks a lot. Much appreciated
How about dosing of mg/kg on humans, outside of standard on-label uses?
I take it 100mg, and general onlabel uses is:
“100 mg PO daily taken before first meal of the day. May increase dose to 300 mg daily if 100 mg/day tolerated in patients who have eGFR ≥60 mL/min…”
So my take is what would be a dosing to have senescence-cleaning effect in human?
Anyway be sure to wash your penis more often when you pee, as there’s a 4-fold increase of fungus and infections due to increase of glucose in urine.
Fabio