Background: Telmisartan, a widely used angiotensin II receptor blocker (ARB) with partial peroxisome proliferator-activated receptor-gamma (PPAR-γ) activity, may confer additional cardiovascular and metabolic benefits. However, evidence comparing telmisartan with other ARBs in terms of major cardiovascular outcomes and risk of new-onset diabetes remains limited
Method: 59767 patients with hypertension and ARB use between January 1, 2007 to December 31, 2017 were identified from the Chang Gung Research Database (CGRD), a multi-institutional electronic medical record database in Taiwan. Patients prescribed telmisartan or other ARBs for at least six months were included. Propensity score matching (1:4) was applied to balance baseline characteristics. Primary outcomes were new-onset diabetes mellitus(DM), major adverse cardiovascular events (MACE) (non-fatal myocardial infarction, non-fatal stroke and CV death) and all cause mortality. Secondary outcomes include hospitalization for heart failure and malignancy. The risks of new-onset DM, MACE, and mortality were compared between two groups using Cox proportional hazards models. In addition, we performed analyzes using Fine and Gray sub-distribution hazard models that considered death a competing risk.
Result: A total of 15,160 patients (telmisartan: 3,032; other ARBs: 12,128) were included after matching. Telmisartan users had a significantly lower risk of 3P-MACE (aHR 0.88, 95% CI 0.80–0.97, p = 0.0074) and non-fatal MI (aHR 0.68, 95% CI 0.52–0.90, p = 0.006) compared to other ARB users. No significant differences were observed for new-onset DM (aHR 1.06, 95% CI 0.88–1.28, p = 0.54), cardiovascular death (aHR 0.86, 95% CI 0.62–1.18, p = 0.35), or other outcomes such as stroke or hospitalization for heart failure.
Conclusion: Telmisartan is associated with superior cardiovascular protection which mainly attributed to reducing risks of non-fatal MI compared to other ARBs, while exhibiting a neutral effect on risk of new-onset DM. These findings suggest telmisartan may be a preferred ARB for hypertensive patients at high cardiovascular risk. Further prospective studies are warranted to validate these results and explore the underlying mechanisms.
There’s a lot of discussion across the forum about various BP meds, and I always forget what the secondary pleiotropic effects of each are, so I made myself a summary. It’d be interesting to see which ones have had positive life-extending results in various animal models (or human association studies).
ARB
Telmisartan - Partial agonist of PPAR-gamma (at >= 80mg) and PPAR-delta. May provide protective benefits for vascular and renal health via PPAR-gamma agonism. Clinical trials have shown that telmisartan increases insulin sensitivity, reduces cardiac fibrosis and hypertrophy, and improves endothilial function.
Losartan - Reduces uric acid levels
Valsartan - Partial agonist of PPAR-gamma (weaker than Telmisartan).
Beta-Blockers
Carvedilol - α1-adrenergic receptor antagonist. Could be helpful for BPH and PTSD.
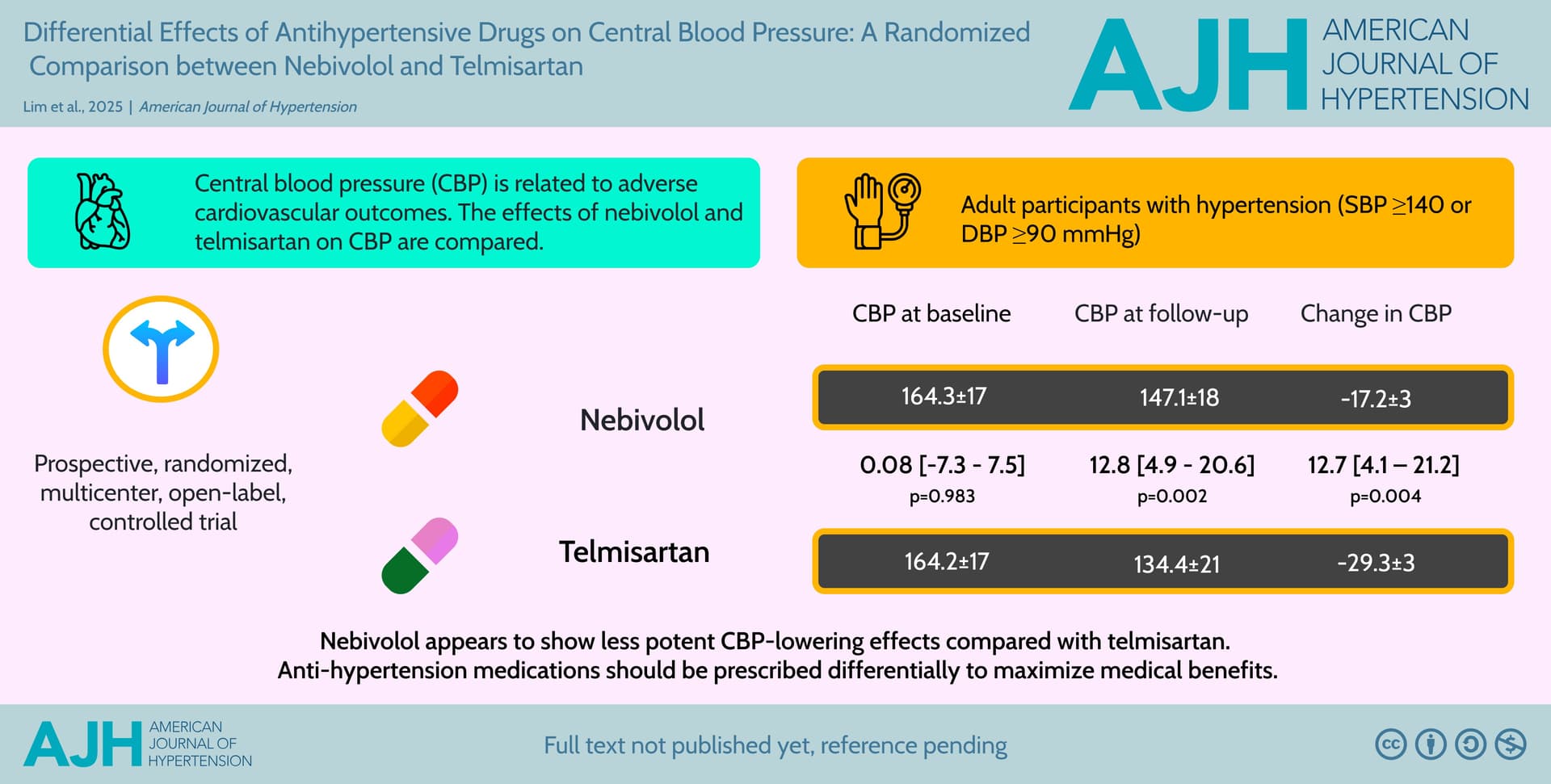
Nebivolol - Nitric oxide potentiator via stimulation of β3 receptors.
Non-dihydropyridine calcium channel blockers - Potentially useful in reducing heart rate increase from GLP-1s.
Good summary. SGLT2i are probably better at reducing uric acid levels than losartan.
DHP CCBs are associated with lower levels of dementia and they extend lifespan in worms.
Terazosin and doxazosin are associated with lower levels of dementia, they extend lifespan in worms.
Beta-blockers (with the potential exception of carvedilol and nebivolol) mess up with glycemic control and are associated with a higher risk of Parkinson’s. They don’t seem neuroprotective against AD.
With this approach, we identified 3 high-confidence FDA-approved candidate drugs for T2D, and validated telmisartan, an anti-hypertensive drug, in our EHR data with over 3 million patients. We found that telmisartan users were associated with a reduced incidence of T2D compared to users of other anti-hypertensive drugs and non-users, supporting the therapeutic potential of telmisartan for T2D. Our framework can be applied to other diseases for translating GWAS findings to aid drug repurposing for complex diseases.
Probably should just use pioglitazone if the goal is T2D improvement. Telmisartan’s activation of PPAR-gamma is certainly a nice additional effect, but I probably wouldn’t reach for it first to improve insulin sensitivity alone in the absence of high blood pressure.
I think most people have suboptimal BP. If your SBP is above 110, I’d say to try Telmisartan 80 mg before pioglitazone. The negative effects of pioglitazone (effects on bone) are too significant to dismiss while the side effects of Telmisartan are trivial as long as your SBP is above 110.
TBH, most people have a SBP way above 120, so the beneficial effects of Telmisartan 80 mg are twofold.
At 5 years, the increment in fracture risk between pioglitazone and placebo groups was 4.9% [13.6% vs 8.8%; hazard ratio (HR), 1.53; 95% confidence interval (CI), 1.24 to 1.89). In each group, ∼80% of fractures were low energy (i.e. , resulted from fall) and 45% were serious (i.e. , required surgery or hospitalization). For serious fractures most likely to be related to pioglitazone (low energy, nonpathological), the risk increment was 1.6% (4.7% vs 3.1%; HR, 1.47; 95% CI, 1.03 to 2.09). Increased risk for any fracture was observed in men (9.4% vs 5.2%; HR, 1.83; 95% CI, 1.36 to 2.48) and women (14.9% vs 11.6%; HR, 1.32; 95% CI, 0.98 to 1.78; interaction P = 0.13).
Yikes. Pretty bad. They also looked at dosing and found that lower doses still had increased fracture risk, though they didn’t specify how much, just that it was less than higher doses. I wonder if there’s a way to counteract this. Perhaps even lower dose (splitting 15mg pills). I guess the question is, why would a partial agonist not have the same issue?
I just recently started Nebivolol, 5 mg, (instead of taking Labetalol), in addition to Amlodipine 2.5 mg and Telmisartan, 40 mg. My BP dropped pretty low - 105/66/51. It’s a big change from 130/80/60. Is it too low now? I’m sure it’s Nebivolol that affects it that much.
No, I don’t have obvious orthostatic symptoms, but I do feel a little lightheaded, either sitting or standing. Not to a degree that I cannot function. Energy is definitely lower than usual. May be I need time to adjust?
I used to suffer from orthostatic hypotension, but that strangely disappeared when I started my blood pressure meds.
“My blood pressure without b.p lowering meds was, at its worst, 147/101.
When I went back onto 10mg Telmisartan and 2.5mg Nebivolol my blood pressure drops to 99/69”
i wondered if as well as bringing my blood pressure down, that it also provided a support to prevent it going too low
….or it might all be just a happy coincidence
PS I’m still going through a bitter divorce, which is why i haven’t posted anything in a while
Telmisartan also reduces blood pressure variability, so perhaps that could explain the improvement in orthostatic intolerance (which is by definition a BP variability problem).
10mg telmisartan seems fairly low dosage. I didn’t realize such dosages were commonly available, the lowest I saw was 20mg. Maybe it’s the Nebivolol doing all the work here.
Compared with less intensive treatment, the risk of orthostatic hypertension was lower with more intensive blood pressure treatment (odds ratio 0.93, 95% confidence interval 0.90 to 0.96). Effects were greater among non-black versus black adults (odds ratio 0.86 v 0.97; P for interaction=0.003) and adults without diabetes versus those with diabetes (0.88 v 0.96; P for interaction=0.05) but did not differ by age ≥75 years, sex, baseline seated blood pressure ≥130/≥80 mm Hg, obesity, stage 3 kidney disease, stroke, cardiovascular disease, standing systolic blood pressure ≥140 mm Hg, or pre-randomization orthostatic hypertension (P for interactions ≥0.05).