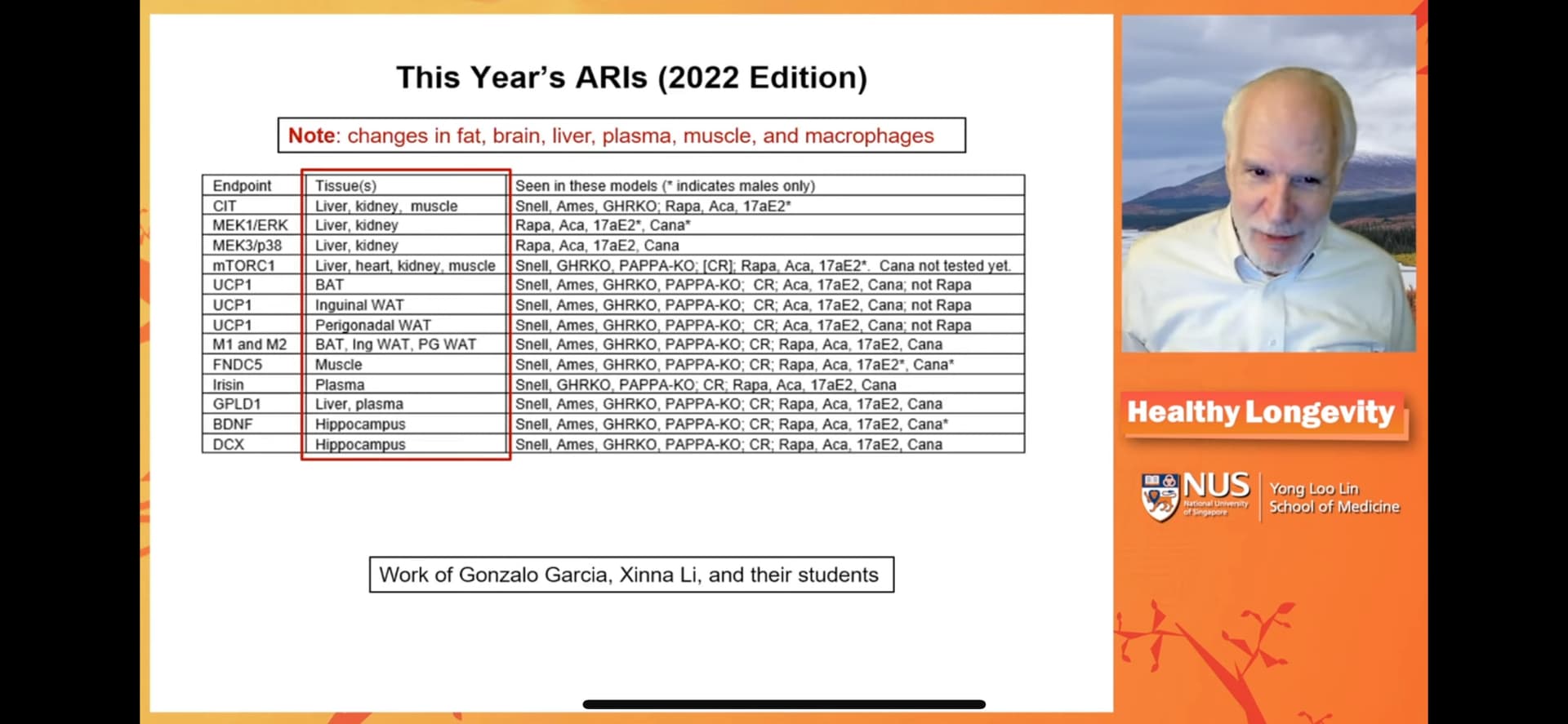
This presentation from Richard Miller goes in depth and compares 9 longevity interventions and what they have in common.

It’s worth watching.
This presentation from Richard Miller goes in depth and compares 9 longevity interventions and what they have in common.
It’s worth watching.
Yes, this is the one I recalled. The discussion starts at 15:20. He says that all of these drugs do tons of things that are not overlapping. Our goal was to focus only on the things they do that are overlapping.
This is part of an effort to be able to identify promising molecules more quickly. Right now the hit rate is only 10–15% on the molecules that they test. I think the thought is that if the new drug has an effect on the areas where these 4 drugs overlap, then they are more likely to extend life span.
I will contact the authors and try to get a copy, and post if I do.
This video is very good. Thanks for posting.
I learned several important facts and educated opinions from Dr Millers presentation. In particular I hadn’t appreciated the importance of multiple interventions vs bigger doses of single interventions to avoid compounding side effects while aiming to compound benefits. Of course spreading interventions across multiple mechanisms is best but even hitting multiple mTOR inhibitors can be superior to bigger doses of any particular drug or lifestyle intervention.
Also, go to 00:57:00 to hear Dr Miller attempt (successfully in my mind) to drive a stake through the heart of the idea that senescent cells are a key driver of aging. He is not just saying fisetin doesn’t work.
Here’s the link just in case you can’t find it above:

Sometimes I do wonder if I am on a fool’s errand with all the supplements I take. So, I am 82 and in good health, but how much of that is due to supplements, and how much is due to diet, exercise, and genes?
I saw this today and it agrees with some of my observations of other people. ![]()
You are wise to wonder about this question. I don’t think you are wasting your time. You might be wasting your money. We should be careful not to injure ourselves of course. That would be a major bummer.
The puzzle of a long healthy life is a hard one. It does engage the brain but you and I will fail to live forever. So what are we aiming for? The meaning of life cant be to live a long time. We want to live a long time in health to accomplish what?
Helping each other (giving and getting) here adds some meaning.
Arthur Brooks has some useful advice, I think.
Could you explain what you found convincing? I listened to that segment, and while I respect his opinion as well informed and scientifically plausible, I don’t see him supporting it here beyond the fisetin results.
He clearly has the view that Senescent cells do not cause aging. I think that the research on transplantation demonstrates that the level of aged (senescent) cells in transplanted organs causes the rest of the organism to age more quickly.
I personally think it is the IL-10 in SASP that causes cells to go senescent. I think a main reason for some cells being senescent is the failure of cells to properly differentiate from being stem cells (and the reason for this is a shortage of acetyl-CoA during the differentiation process.) I think they are basically cells that are stuck in the differentiation process.
Hence you get more senescent cells in areas with more cell growth.
IMO The other main pathway is that of mitochondrial efficiency which also affects acetyl-CoA levels, but also affects ATP availability for translation of mRNA into protein.
Here are my notes regarding Dr Millers discussion of scenescent cells:
Millers opinion with Dr Kennedy’s agreement as described below.
I understand miller to say that the basis of thinking that scenescent cells IS a driver of aging is not based on good science. And he is clearly saying his opinion is that scenescent cells are not a key driver of aging.
I do not think he has proof, but is saying no one has proof of the original proposition so he’ll wait for that to emerge (and doubts it will emerge).
I’ll wait as well.
Thanks. There is a world of difference between the statements “Cellular senescence isn’t proven to be a major factor in aging” and “cellular senescence isn’t a major factor in aging”. The second claim needs support.
I understand what you are saying. But it’s hard to prove a negative. The onus has to be on the scientists saying scenescent cells are a major cause of aging …for them to show evidence of it. That’s what I think.
The good news is that whether you believe senescent cells are beneficial for longevity or not if you are taking Rapamycin, you are inhibiting senescent cell formation anyway. Same with taurine, metformin, and NAC. I still believe that senescent cells are not healthy for you and I’m happy to take anything to prevent them even though it may affect wound healing. To be honest, I don’t think senescent cells are going to slow down cancer enough to make a difference. If that were true, smokers, who have a lot of senescent cells would have a lower incidence/progression of cancer and that just isn’t so. The senescent cells helps against cancer argument just doesn’t hold water for me.
Senescence is a double-edged sword that can function in opposite directions. It is a potential mechanism for a cell to avoid malignant transformation. However, senescence can also promote cancer development by altering the cellular microenvironment through a senescence-associated secretory phenotype (SASP).