I’m not challenging the outcome of the study. My point is that the number of targeted receptors has no bearing on a weight-loss drug being better than one with fewer targeted receptors. Each drug has an objective and each person has a goal. And that’s what will determine which drug is better for each person. Weight loss percentage over a given time is a single measure.
If my weight-loss goal included minimizing the loss of lean muscle mass, I would likely choose Pemvidutide, a 2 receptor agonist.
If I were a bodybuilder who had difficulty adding weight during a bulking cycle, I would choose Reta at a low dose to increase my appetite.
If I were “skinny fat”, I would choose Reta to obliterate my visceral fat.
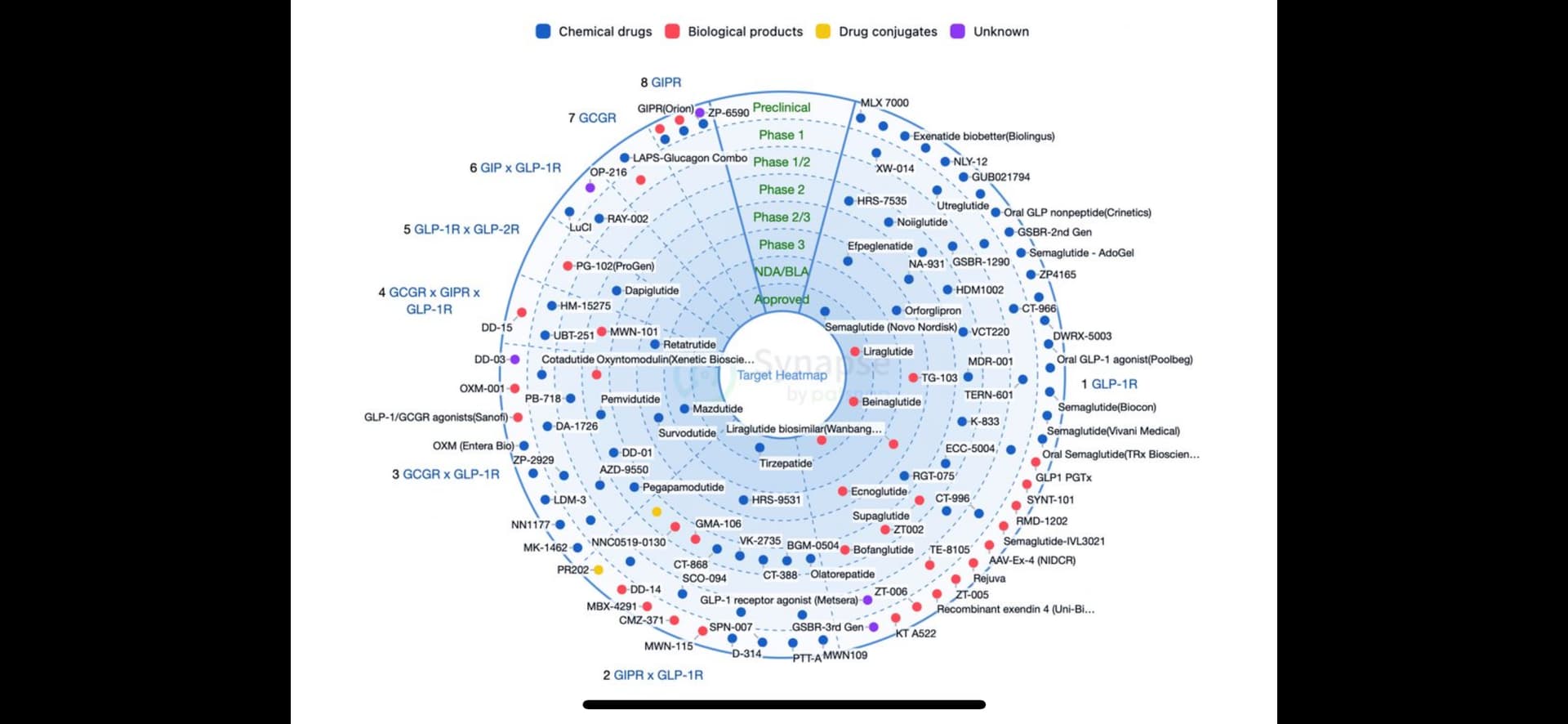
This chart is 2 weeks old and shows weight-loss drugs by targeted receptor and trial class.
The choices I would consider making for myself, given each of the scenarios, are based on clinical studies in humans. The second scenario is based on clinical studies and “research” completed by others that has been shared with me.
I hope you’re right that it has a lean mass sparing effect, but I haven’t yet seen any human clinical data for retatrutide’s effect on body composition (only on overall weight loss). Have you also seen/heard that reta often increases heart rate more than sema/tirz?
My RHR has not changed since I started Tz or Rt and neither has my HRV been negatively affected, Same for the boss
We measure both every day as soon as we wake up. I use the EliteHRV app and their finger clip (discontinued).
Been doing that consistently for 4 years as part of our vagus nerve stimulation program using a TENs unit and ear clip. I’ve posted a PDF with a DIY how to here, Might help those who do experience changes in RHR and HRV when taking these drugs.
My previous post states Pemvidutide, not Reta, is muscle sparing during weight loss per clinical trials. Yes, rise in heart rate is a potential side effect with Reta.
Ok, but you said a bodybuilder could use low dose reta to increase appetite during bulking phase, so that’s what I meant by lean mass sparing. You’re saying at low dose, appetite would be increased above baseline while lean mass not negatively affected, while at the same time preventing as much fat gain that would normally occur during bulking?
My 40 y/o son works out pretty hard and has a physical job. He’s a beast. He goes to the gym at 4:00am and is in bed by 8:00pm. He has an appetite! and lives with us so he is participating in many of our little experiments.
A month ago he asked if he could try low dose Rt and started on 1mg a week. He’s found new control over his appetite and has not lost any muscle while dropping 7lb (currently 185 down from 192). He has a Withings Body Cardio scale like ours and weighs himself 3 to 4 days a week. It measures weight, water, fat, bone, muscle, and does PWV. According to that scale he has not lost any muscle.
I have a “theory” on muscle loss related to GLP1-R use.
My “theory” on muscle loss comes from being a butcher when I was a kid.
Long story short, we had a small local beef operation, a slaughter house, a meat market and did custom cutting and freezing. From 13 to 19, I worked in that operation every day, after school, weekends, holidays??? I’ve “dissected” a lot of animals, cattle, pigs, lambs! We used to also serve local hunters, deer, moose and bear have been under my knife. I used to raise a competition cow for 4-H every year and sell it at auction. The objective was the fatter the better. Healthy, well marbled beef was the goal
Fat marbling is not exclusive to cattle. Humans can acquire a lot of inter-muscular fat.
My theory is the muscle “shrinkage” often seen with ANY weight loss, not just GLP1-R’s is probably exacerbated by the loss of this inter-muscular fat which will shrink the overall size of the muscle (and thereby the muscle “weight”) but have minimal effect on the total muscle fibres themselves.
Take all the fat out of a piece of Wagyu and see what’s left of the muscle, compare that to the leanness of Texas Longhorn.
Just a theory and this may have already been thoroughly sorted out by the folks who wear the lab coats.
I could have been clearer in my scenarios and it was not my intent to imply that a negative side effect that some have experienced will apply to everyone. Reta speeds up the metabolism and increased appetite at low dose can be a side effect. Some BBs are taking advantage of this. I’m on multiple platforms to better educate myself and these are unexpected, recurrent outcomes.
In the post from Steve_Combi, his son is experiencing appetite suppression at a low dose of Reta so his experience is different than the scenario in my post. Others find that they need to stack Tirz or Sema or Cagrilintide with Reta to provide additional appetite suppression at lower Reta doses.
Weight loss is a secondary benefit for which these drugs were originally designed. The use of these drugs as well as combinations of these drugs will continue to be studied/trialed for other benefits beyond diabetes and obesity.
Off-hand, though I would suggest stockpiling anyways because there are now MULTIPLE risks (I hope Elon can convince everyone that we need this - as he has tweeted that it’s the single most important thing for health - despite RFK Jr speaking out against ozempic/tirzepatide/etc). And who knows if the Trump admin will get corrupt again.
btw I was at a retatrutide injection party with a few people a few days ago. There were some nausea side effects reported but nothing major (they were fine after). alas they didn’t let me inject retatrutide (oh well, I’ll drink A LOT of almond milk over the next few days instead)